

Bone age advancement in prepubertal children with obesity and premature adrenarche: possible potentiating factors
- PMID: 21311512
- PMCID: PMC3637026
- DOI: 10.1038/oby.2010.305
Bone age advancement in prepubertal children with obesity and premature adrenarche: possible potentiating factors
Abstract
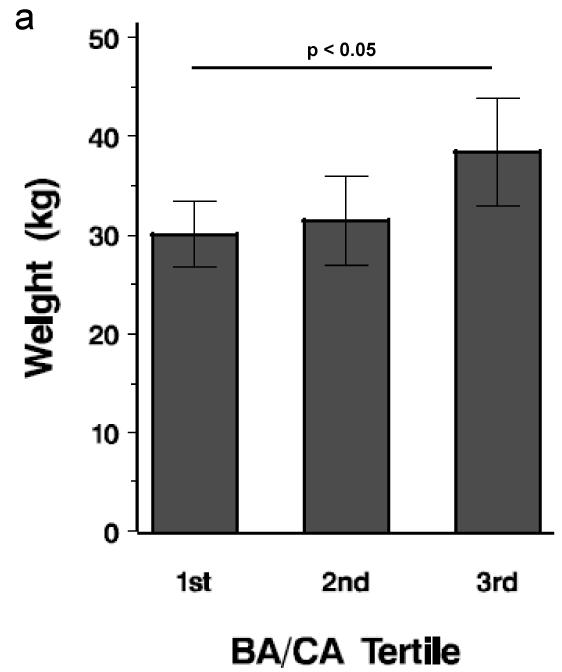
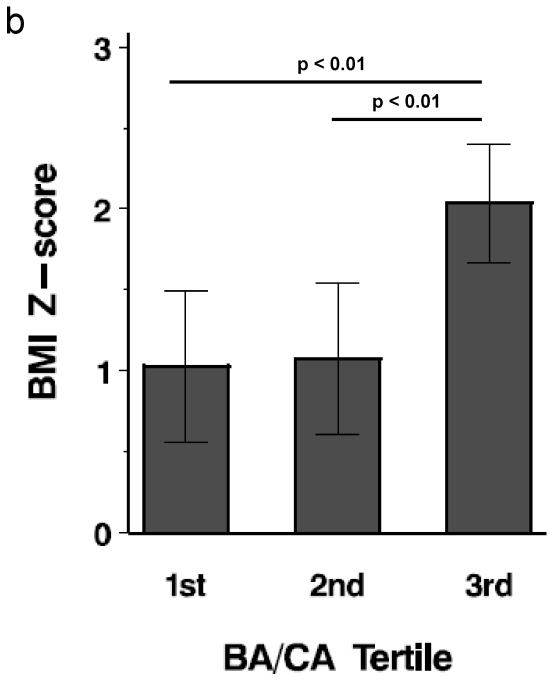
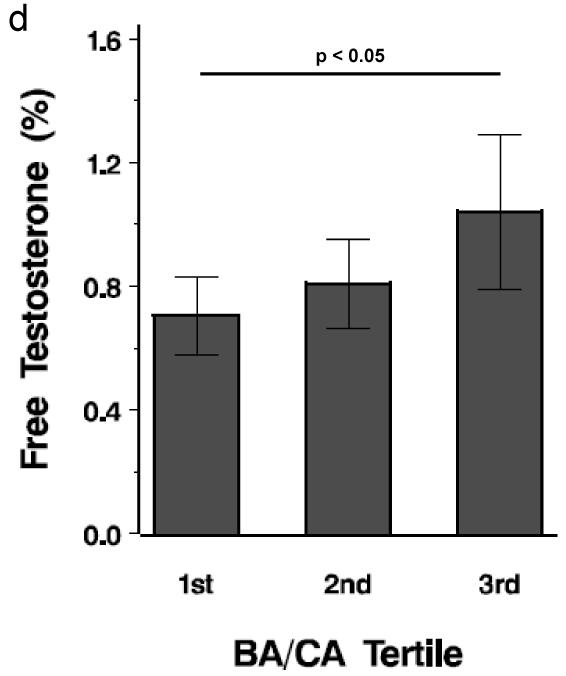
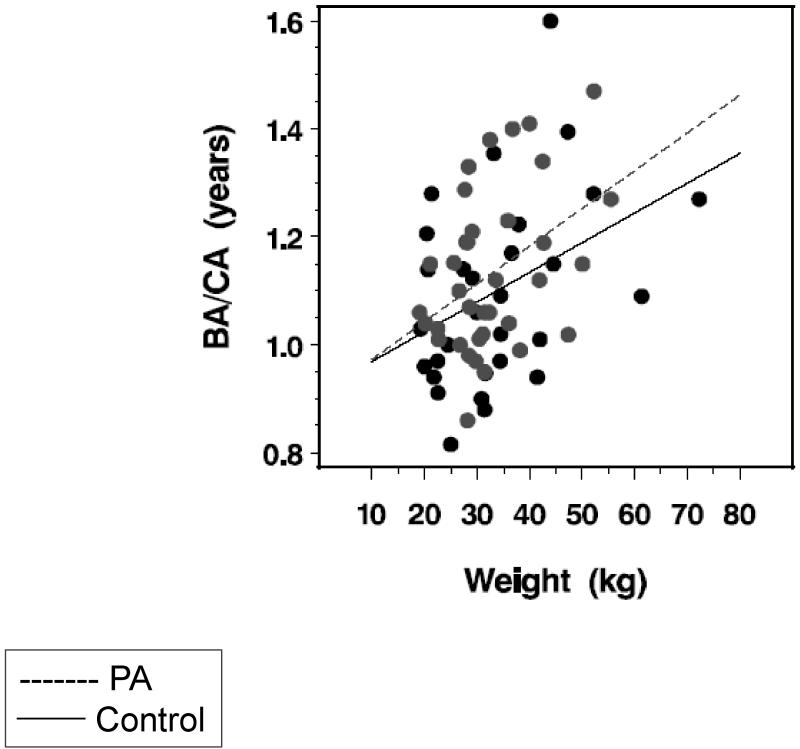
Obesity and premature adrenarche (PA) are both associated with bone age (BA) advancement of unclear etiology, which may lead to earlier puberty, suboptimal final height and obesity in adulthood. Our objective was to understand the hormonal and anthropometric characteristics of BA advancement in a spectrum of prepubertal children with and without obesity and PA. In this cross-sectional study of 66 prepubertal children (35 PA, 31 control, 5-9 years), BMI z-score, hormonal values and response to an oral glucose tolerance test were the main outcome measures. Subjects were divided into tertiles by BA divided by chronological age (BA/CA), an index of BA advancement. Subjects in the top tertile for BA/CA had the highest dehydroepiandrosterone sulfate (DHEAS), free testosterone (%), hemoglobin A(1C), BMI z-score, and weight (P < 0.05). BMI z-score (r = 0.47), weight (r = 0.40), free testosterone (%) (r = 0.34), and DHEAS (r = 0.30) correlated with BA/CA (P < 0.02). Regression analysis showed greater BA/CA in PA compared to controls after controlling for weight (0.21 ± 0.56, P < 0.004). An exploratory stepwise regression model showed that weight, estradiol, and DHEAS were the strongest predictors of BA/CA accounting for 24% of its variance. Obesity was highly associated with BA advancement in this study of prepubertal children. In addition, children with PA had greater BA/CA at any given weight when compared to controls. These findings suggest a possible hormonal factor, which potentiates the effect of obesity on BA advancement in children with obesity and/or PA.
Figures

References
-
- Korth-Schutz A, Levine LS, New MI. Evidence for the adrenal source of androgens in precocious adenarche. Acta Endocrinol (Copenh) 1976;82:242–252. - PubMed
-
- Ibanez L, Jimenez R, Zegher F. Early puberty-menarche after precocious pubarche: relation to prenatal growth. Pediatrics. 2006;117:117–121. - PubMed
-
- Diaz A, Bhandari S, Sison C, Vogiatzi M. Characteristics of children with premature pubarche in the New York Metropolitan Area. Horm Res. 2008;70:150–154. - PubMed
-
- Ibanez L, Verdis R, Potau N, Zampolli M, Ghizzoni L, Albisu MA, et al. Natural history of premature pubarche: an auxological study. J Clin Endocrinol Metab. 1992;74:254–257. - PubMed
-
- Utriainen P, Voutilainen R, Jaaskelainen J. Girls with premature adrenarche have accelerated early childhood growth. J Pediatr. 2009;154:882–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
