

Comparison of outcomes with multifocal intraocular lenses: a meta-analysis
- PMID: 21311656
- PMCID: PMC3033003
- DOI: 10.2147/OPTH.S14325
Comparison of outcomes with multifocal intraocular lenses: a meta-analysis
Abstract
Purpose: To compare the clinical outcome of different multifocal intraocular lenses (IOLs) based on information reported in the international literature.
Methods: All comparative clinical trials that involved implanting at least one multifocal IOL in patients with cataract or presbyopia were extracted from the literature. Clinical outcomes included uncorrected near visual acuity, uncorrected distance visual acuity, visual acuity, spectacle independence, and halos. Random effects meta-analyses were conducted to compare outcomes for the different IOL types.
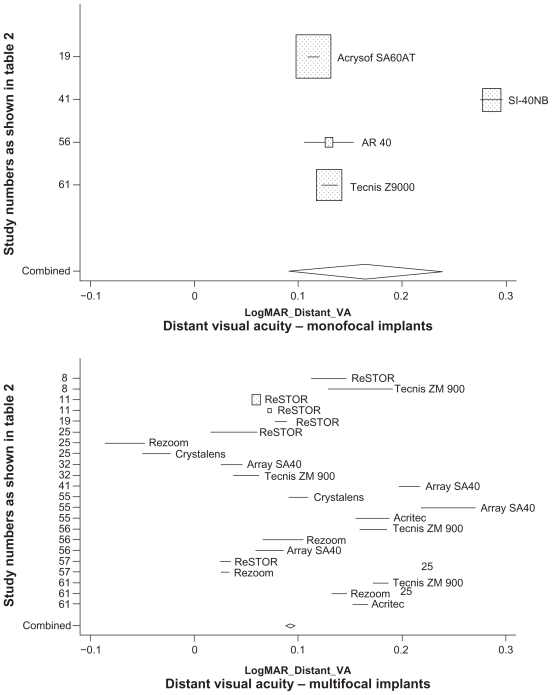
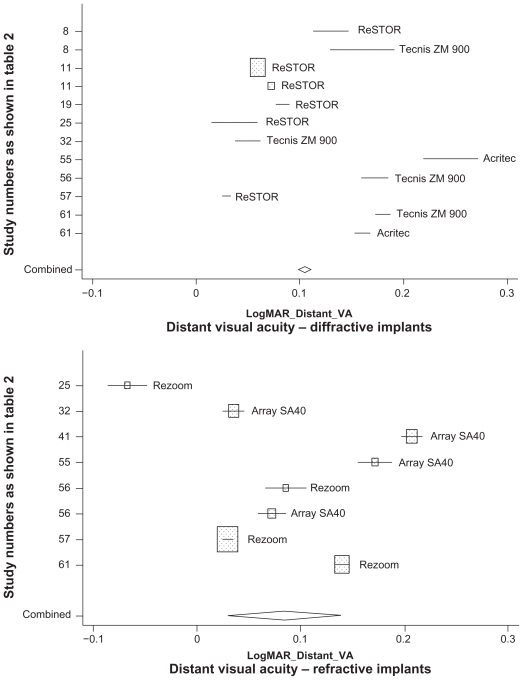
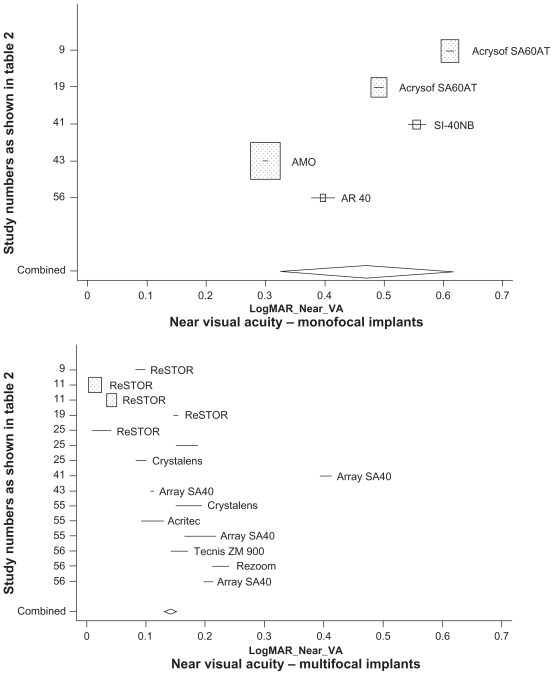
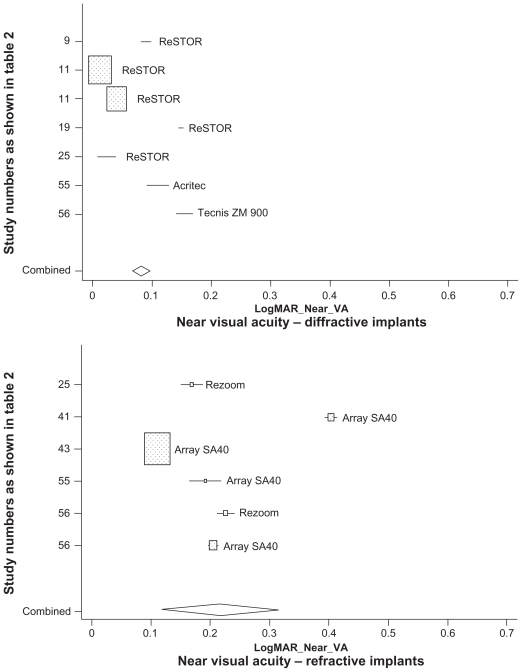
Results: Twenty papers were identified describing 11 monofocal IOLs and 35 multifocal IOLs (19 diffractive, including 12 ReSTOR(®), 14 refractive, and two accommodative) patient cohorts. Multifocal and monofocal uncorrected distance visual acuity was 0.165 (0.090-0.240) and 0.093 (0.088-0.098), respectively. Compared with monofocal IOLs, multifocal IOLs produced better uncorrected near visual acuity (0.470 [0.322-0.618] versus 0.141 [0.131-0.152]; P < 0.0001), resulting in higher spectacle independence (incidence rate ratio [IRR] 3.62 [2.90-4.52]; P < 0.0001). Compared with refractive multifocal IOLs, diffractive multifocal IOLs produced a similar uncorrected distance visual acuity (0.105 [0.098-0.111] versus 0.085 [0.029-0.140]; P ≤ 0.78, not significant) and better uncorrected near visual acuity (0.217 [0.118-0.317] versus 0.082 [0.067-0.098]; P < 0.0001) resulting in higher spectacle independence (IRR 1.75 [1.24-2.48]; P < 0.001). Compared with other multifocal IOLs, ReSTOR produced a better uncorrected distance visual acuity (0.067 [0.059-0.076] versus 0.093 [0.088-0.098]; P < 0.0001) and better uncorrected near visual acuity (0.064 [0.046-0.082] versus 0.141 [0.131-0.152]; P < 0.006), resulting in higher spectacle independence (IRR 2.06 [1.26-1.36]; P < 0.004). Halo incidence rates with different types of multifocal implants did not differ significantly.
Conclusion: Multifocal IOLs provide better uncorrected near visual acuity than monofocal IOLs, leading to less need for spectacles. Multifocal IOL design might play a role in postsurgical outcome, because better results were obtained with diffractive lenses. ReSTOR showed better uncorrected near visual acuity, uncorrected distance visual acuity, and higher spectacle independence rates compared with other multifocal IOLs.
Keywords: meta-analysis; multifocal implants; patient satisfaction; spectacle independence; uncorrected distance visual acuity; uncorrected near visual acuity.
Figures
References
-
- Congdon N, Vingerling JR, Klein BE, et al. Prevalence of cataract and pseudophakia/aphakia among adults in the United States. Arch Ophthalmol. 2004;122:487–494. - PubMed
-
- Javitt JC, Wang F, West SK. Blindness due to cataract: Epidemiology and prevention. Ann Rev Public Health. 1996;17:159–177. - PubMed
-
- Agency for Health Care Policy and Research. Cataract in Adults: Management of functional impairment. Rockville, MD: Agency for Health Care Policy and Research; 1993.
-
- Anmarkrund N, Bergaust B, Bulie T, Sand AB. Evaluation of a flexible one-piece open-loop anterior chamber lens Symflex 350B 3–4 years after implantation. Acta Ophthalmol. 1993;71:796–800. - PubMed
-
- Pötzsch DK, Lösch-Pötzsch M. Four year follow-up of the Memorylens. J Cataract Refract Surg. 1996;22:1336–1341. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
