

Refractory chronic lymphocytic leukemia--new therapeutic strategies
- PMID: 21317446
- PMCID: PMC3248129
- DOI: 10.18632/oncotarget.184
Refractory chronic lymphocytic leukemia--new therapeutic strategies
Abstract
Treatment outcome of chronic lymphocytic leukemia (CLL) has considerably improved since the introduction of fludarabine (F) as part of the standard therapy. Nevertheless, refractoriness to fludarabine occurs in a significant number of patients and is associated with an unfavorable prognosis. Important risk factors are 17p deletion and/or mutation of TP53. For this subgroup the CD52 antibody alemtuzumab (A) presents a new treatment approach and has already been approved. Meanwhile we have to face also refractoriness to alemtuzumab. Importantly, the monoclonal CD20 antibody ofatumumab has now shown efficacy in F and A double-refractory CLL. The next generation CD20 antibody GA-101 is currently compared to rituximab (R) and will possibly be its more potent successor. Further B-cell antigens are targeted by lumiliximab (CD23), TRU-016 (CD37) and blinatumomab (CD19). Apart from monoclonal antibody therapies, a great number of small molecules are examined for the treatment of refractory and relapsed CLL. Most of these agents aim to overcome apoptosis resistance in CLL cells or influence the microenvironment. Typical targets are regulators of the cell cycle and antiapoptotic molecules like the members of the Bcl-2 family. Up to now the most promising agents appear to be flavopiridol and lenalidomide among others.
Figures
Comment in
-
Phosphoinositide 3'-kinase delta: turning off BCR signaling in Chronic Lymphocytic Leukemia.Oncotarget. 2011 Oct;2(10):737-8. doi: 10.18632/oncotarget.341. Oncotarget. 2011. PMID: 22006556 Free PMC article.
References
-
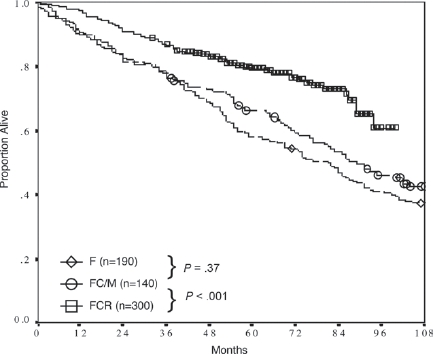
- Hallek M, Fischer K, Fingerle-Rowson G, Fink A-M, Busch R, Mayer J, Hensel M, Hopfinger G, Hess G, Von Gruenhagen U, Bergmann M, Catalano J, Zinzani PL, Caligaris-Cappio F, Seymour JF, Berrebi A, Jäger U, Cazin B, Trneny M, Westermann A, Wendtner CM, Eichhorst B, Staib P, Bühler A, Winkler D, Zenz T, Böttcher S, Ritgen M, Mendila M, Kneba M, Döhner H, Stilgenbauer S. Addition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocytic leukemia: a randomised, open-label, phase 3 trial. Lancet. 2010 in press. - PubMed
-
- Keating MJ, O'Brien S, Lerner S, Koller C, Beran M, Robertson LE, Freireich EJ, Estey E, Kantarjian H. Long-term follow-up of patients with chronic lymphocytic leukemia (CLL) receiving fludarabine regimens as initial therapy. Blood. 1998;92:1165–1171. - PubMed
-
- Rai KR, Peterson BL, Appelbaum FR, Kolitz J, Elias L, Shepherd L, Hines J, Threatte GA, Larson RA, Cheson BD, Schiffer CA. Fludarabine compared with chlorambucil as primary therapy for chronic lymphocytic leukemia. N Engl J Med. 2000;343:1750–1757. - PubMed
-
- Catovsky D, Richards S, Matutes E, Oscier D, Dyer MJ, Bezares RF, Pettitt AR, Hamblin T, Milligan DW, Child JA, Hamilton MS, Dearden CE, Smith AG, Bosanquet AG, Davis Z, Brito-Babapulle V, Else M, Wade R, Hillmen P. Assessment of fludarabine plus cyclophosphamide for patients with chronic lymphocytic leukaemia (the LRF CLL4 Trial): a randomised controlled trial. Lancet. 2007;370:230–239. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
