

Incidence and risk factors of recurrent acute lung injury
- PMID: 21317648
- PMCID: PMC3102133
- DOI: 10.1097/CCM.0b013e31820edf91
Incidence and risk factors of recurrent acute lung injury
Abstract
Objective: To determine risk factors for development of recurrent acute lung injury.
Design: A population-based case-control study.
Setting: The study was conducted in Olmsted County, MN, from 1999 to 2008.
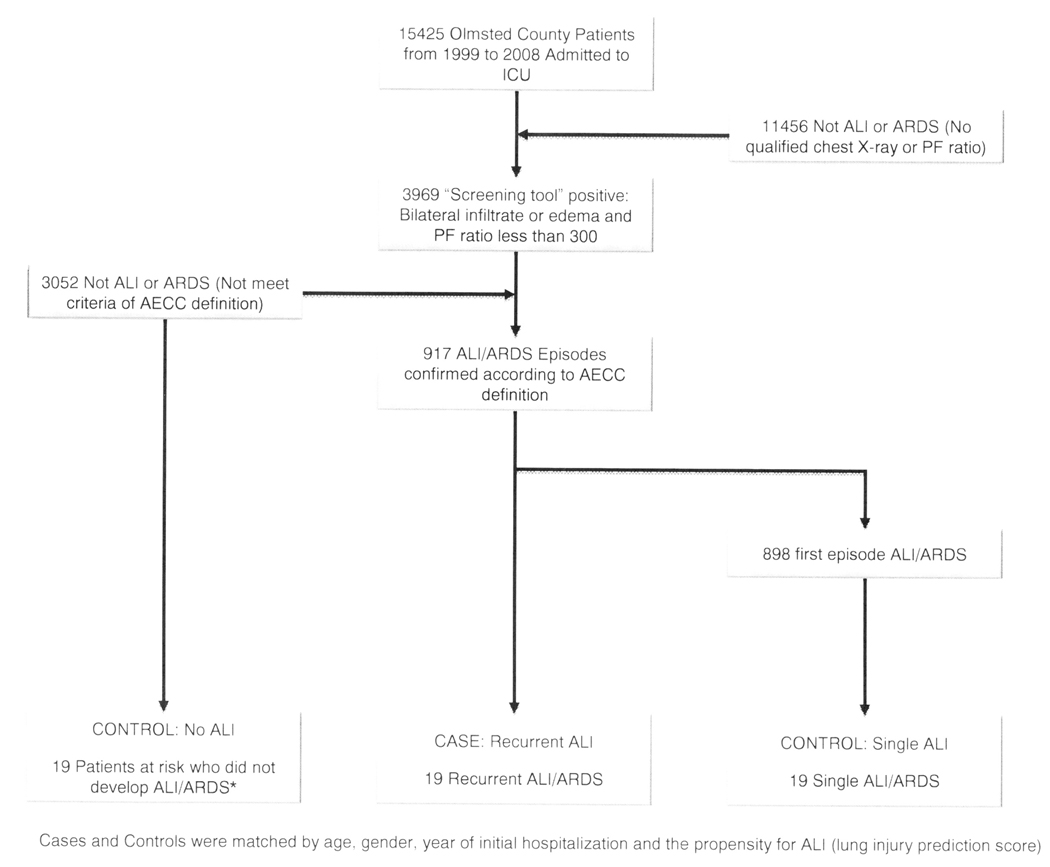
Patients: Using a validated electronic screening protocol, investigators identified intensive care patients with acute hypoxemia and bilateral pulmonary infiltrates.
Interventions: None.
Measurements and main results: The presence of acute lung injury was independently confirmed according to American-European Consensus Conference criteria. Recurrent acute lung injury cases were subsequently matched (1:1:1) with two controls (single acute lung injury and no acute lung injury) on age, gender, duration of follow-up, and predisposing conditions. Risk factors evaluated included gastroesophageal reflux disease, alcohol consumption, smoking, chronic opioid use, and transfusions. We identified 917 patients with acute lung injury, 19 of which developed a second episode, yielding a frequency of 2.02 (95% confidence interval 1.10-2.93) per 100,000 person years. The median time to development of the second episode was 264 days (interquartile range 80-460 days), with a mortality of 47% during the episode. The history of gastroesophageal reflux disease was highly prevalent in patients who developed recurrent acute lung injury: 15 of 19 patients (79%) compared to 5 of 19 (26%) matches with a single episode of acute lung injury (p = .006) and 8 of 19 (42%) matches without acute lung injury (p = .016). Other exposures were similar between the cases and the two matched controls.
Conclusions: Recurrent acute lung injury is not a rare phenomenon in the intensive care unit and may continue to increase with improvements in survival following acute lung injury. Gastroesophageal reflux disease was identified as an important risk factor for recurrent acute lung injury and may suggest an important role of gastric aspiration in the development of this syndrome.
Conflict of interest statement
The other authors have not disclosed any potential conflicts of interest.
Figures
Comment in
-
Page the critical care epidemiologist, STAT!Crit Care Med. 2011 May;39(5):1219-20. doi: 10.1097/CCM.0b013e31821487e2. Crit Care Med. 2011. PMID: 21610586 Free PMC article. No abstract available.
References
-
- Fowler AA, Hamman RF, Good JT, Benson KN, Baird M, Eberle DJ, Petty TL, Hyers TM. Adult respiratory distress syndrome: risk with common predispositions. Ann Intern Med. 1983;98(5 Pt 1):593–597. - PubMed
-
- Gong MN, Thompson BT, Williams P, Pothier L, Boyce PD, Christiani DC. Clinical predictors of and mortality in acute respiratory distress syndrome: potential role of red cell transfusion. Critical care medicine. 2005;33(6):1191–1198. - PubMed
-
- Hudson LD, Milberg JA, Anardi D, Maunder RJ. Clinical risks for development of the acute respiratory distress syndrome. American journal of respiratory and critical care medicine. 1995;151(2 Pt 1):293–301. - PubMed
-
- Pepe PE, Potkin RT, Reus DH, Hudson LD, Carrico CJ. Clinical predictors of the adult respiratory distress syndrome. Am J Surg. 1982;144(1):124–130. - PubMed
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1334–1349. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
