

Aberrantly glycosylated IgA1 as a factor in the pathogenesis of IgA nephropathy
- PMID: 21318178
- PMCID: PMC3034910
- DOI: 10.1155/2011/470803
Aberrantly glycosylated IgA1 as a factor in the pathogenesis of IgA nephropathy
Abstract
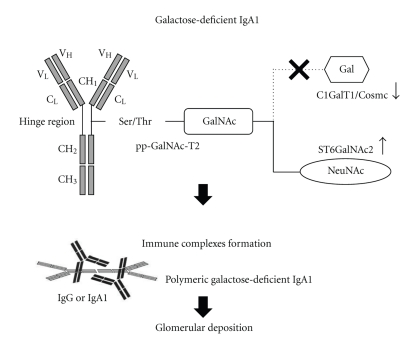
Predominant or codominant immunoglobulin (Ig) A deposition in the glomerular mesangium characterizes IgA nephropathy (IgAN). Accumulated glomerular IgA is limited to the IgA1 subclass and usually galactose-deficient. This underglycosylated IgA may play an important role in the pathogenesis of IgAN. Recently, antibodies against galactose-deficient IgA1 were found to be well associated with the development of IgAN. Several therapeutic strategies based on corticosteroids or other immunosuppressive agents have been shown to at least partially suppress the progression of IgAN. On the other hand, several case reports of kidney transplantation or acquired IgA deficiency uncovered a remarkable ability of human kidney to remove mesangial IgA deposition, resulting in the long-term stabilization of kidney function. Continuous exposure to circulating immune complexes containing aberrantly glycosylated IgA1 and sequential immune response seems to be essential in the disease progression of IgAN. Removal of mesangial IgA deposition may be a challenging, but fundamental approach in the treatment of IgAN.
Figures
Similar articles
-
Pathogenic role of IgA receptors in IgA nephropathy.Contrib Nephrol. 2007;157:64-9. doi: 10.1159/000102306. Contrib Nephrol. 2007. PMID: 17495439 Review.
-
IgA nephropathy and Henoch-Schoenlein purpura nephritis: aberrant glycosylation of IgA1, formation of IgA1-containing immune complexes, and activation of mesangial cells.Contrib Nephrol. 2007;157:134-8. doi: 10.1159/000102455. Contrib Nephrol. 2007. PMID: 17495451 Review.
-
Both IgA nephropathy and alcoholic cirrhosis feature abnormally glycosylated IgA1 and soluble CD89-IgA and IgG-IgA complexes: common mechanisms for distinct diseases.Kidney Int. 2011 Dec;80(12):1352-63. doi: 10.1038/ki.2011.276. Epub 2011 Aug 24. Kidney Int. 2011. PMID: 21866091
-
Glucocorticoids Reduce Aberrant O-Glycosylation of IgA1 in IgA Nephropathy Patients.Kidney Blood Press Res. 2018;43(2):350-359. doi: 10.1159/000487903. Epub 2018 Mar 6. Kidney Blood Press Res. 2018. PMID: 29529610
-
IgA glycosylation and IgA immune complexes in the pathogenesis of IgA nephropathy.Semin Nephrol. 2008 Jan;28(1):78-87. doi: 10.1016/j.semnephrol.2007.10.009. Semin Nephrol. 2008. PMID: 18222349 Free PMC article. Review.
Cited by
-
Serum galactose-deficient IgA1 levels in children with IgA nephropathy.Int J Clin Exp Med. 2015 May 15;8(5):7861-6. eCollection 2015. Int J Clin Exp Med. 2015. PMID: 26221341 Free PMC article.
-
Gluten exacerbates IgA nephropathy in humanized mice through gliadin-CD89 interaction.Kidney Int. 2015 Aug;88(2):276-85. doi: 10.1038/ki.2015.94. Epub 2015 Mar 25. Kidney Int. 2015. PMID: 25807036
-
IgA1 Protease Treatment Reverses Mesangial Deposits and Hematuria in a Model of IgA Nephropathy.J Am Soc Nephrol. 2016 Sep;27(9):2622-9. doi: 10.1681/ASN.2015080856. Epub 2016 Feb 5. J Am Soc Nephrol. 2016. PMID: 26850635 Free PMC article.
-
Bacterial IgA protease-mediated degradation of agIgA1 and agIgA1 immune complexes as a potential therapy for IgA Nephropathy.Sci Rep. 2016 Aug 3;6:30964. doi: 10.1038/srep30964. Sci Rep. 2016. PMID: 27485391 Free PMC article.
-
Clinical and pathological findings of IgA nephropathy following SARS-CoV-2 infection.Clin Exp Med. 2024 Feb 24;24(1):43. doi: 10.1007/s10238-023-01271-2. Clin Exp Med. 2024. PMID: 38400937 Free PMC article.
References
-
- Berger J, Hinglais N. Les depots intercapillaires d’IgA-IgG. Journal d'Urologie et de Nephrology. 1968;74(9):694–695. (Fre). - PubMed
-
- D’Amico G. The commonest glomerulonephritis in the world: IgA nephropathy. Quarterly Journal of Medicine. 1987;64(245):709–727. - PubMed
-
- Galla JH. Iga nephropathy. Kidney International. 1995;47(2):377–387. - PubMed
-
- D’Amico G, Colasanti G, Barbiano di Belgioioso G, et al. Long-term follow-up of IgA mesangial nephropathy: clinico-histological study in 374 patients. Seminars in Nephrology. 1987;7(4):355–358. - PubMed
-
- Radford MG, Donadio JV, Bergstralh EJ, Grande JP. Predicting renal outcome in IgA nephropathy. Journal of the American Society of Nephrology. 1997;8(2):199–207. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous