

Anti-platelet therapy: cyclo-oxygenase inhibition and the use of aspirin with particular regard to dual anti-platelet therapy
- PMID: 21320154
- PMCID: PMC3195738
- DOI: 10.1111/j.1365-2125.2011.03943.x
Anti-platelet therapy: cyclo-oxygenase inhibition and the use of aspirin with particular regard to dual anti-platelet therapy
Abstract
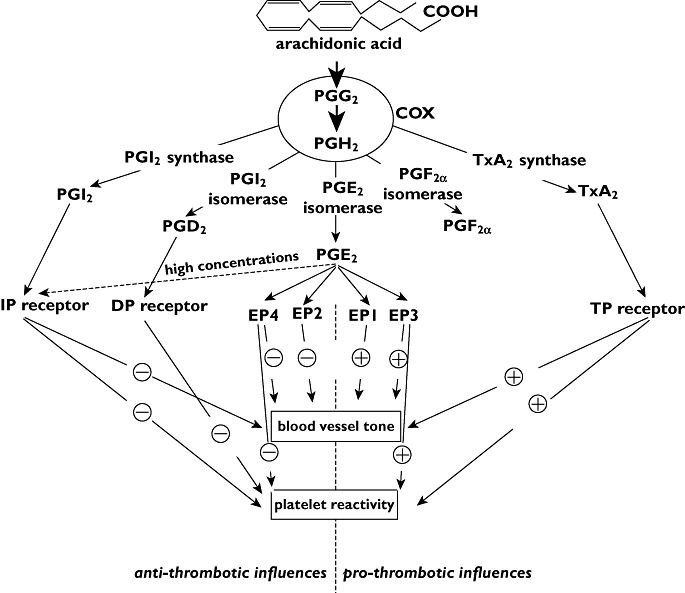
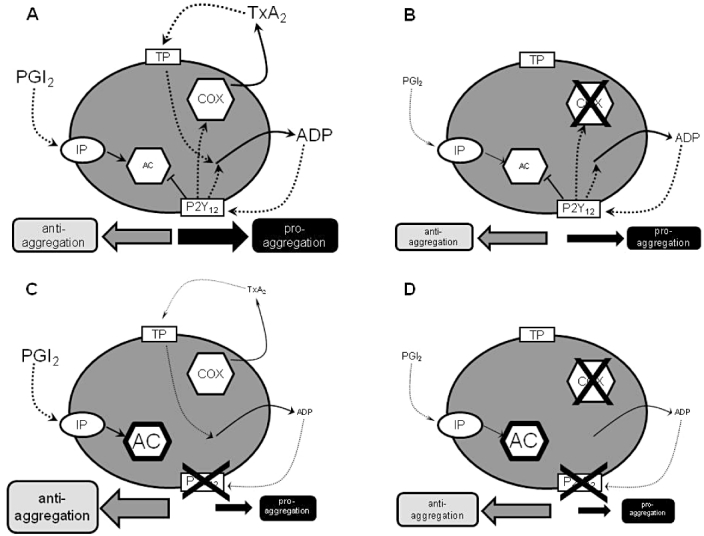
Aspirin and P2Y(12) antagonists are commonly used anti-platelet agents. Aspirin produces its effects through inhibition of thromboxane A(2) (TXA(2)) production, while P2Y(12) antagonists attenuate the secondary responses to ADP released by activated platelets. The anti-platelet effects of aspirin and a P2Y(12) antagonist are often considered to be separately additive. However, there is evidence of an overlap in effects, in that a high level of P2Y(12) receptor inhibition can blunt TXA(2) receptor signalling in platelets and reduce platelet production of TXA(2). Against this background, the addition of aspirin, particularly at higher doses, could cause significant reductions in the production of prostanoids in other tissues, e.g. prostaglandin I(2) from the blood vessel wall. This review summarizes the data from clinical studies in which dose-dependent effects of aspirin on prostanoid production have been evaluated by both plasma and urinary measures. It also addresses the biology underlying the cardiovascular effects of aspirin and its influences upon prostanoid production throughout the body. The review then considers whether, in the presence of newer, more refined P2Y(12) receptor antagonists, aspirin may offer less benefit than might have been predicted from earlier clinical trials using more variable P2Y(12) antagonists. The possibility is reflected upon, that when combined with a high level of P2Y(12) blockade the net effect of higher doses of aspirin could be removal of anti-thrombotic and vasodilating prostanoids and so a lessening of the anti-thrombotic effectiveness of the treatment.
© 2011 The Authors. British Journal of Clinical Pharmacology © 2011 The British Pharmacological Society.
Figures
References
-
- Patrono C, Baigent C. Low-dose aspirin, coxibs, and other NSAIDS: a clinical mosaic emerges. Mol Interv. 2009;9:31–9. - PubMed
-
- Vane JR, Bakhle YS, Botting RM. Cyclooxygenases 1 and 2. Annu Rev Pharmacol Toxicol. 1998;38:97–120. - PubMed
-
- Mitchell JA, Warner TD. COX isoforms in the cardiovascular system: understanding the activities of non-steroidal anti-inflammatory drugs. Nat Rev Drug Discov. 2006;5:75–86. - PubMed
-
- Warner TD, Mitchell JA. Cyclooxygenases: new forms, new inhibitors, and lessons from the clinic. FASEB J. 2004;18:790–804. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
