

Smoking and risk of amyotrophic lateral sclerosis: a pooled analysis of 5 prospective cohorts
- PMID: 21320987
- PMCID: PMC3319086
- DOI: 10.1001/archneurol.2010.367
Smoking and risk of amyotrophic lateral sclerosis: a pooled analysis of 5 prospective cohorts
Abstract
Background: Cigarette smoking has been proposed as a risk factor for amyotrophic lateral sclerosis (ALS), but epidemiological studies supporting this hypothesis have been small and mostly retrospective.
Objective: To prospectively examine the relation between smoking and ALS in 5 well-established large cohorts.
Design: Five prospective cohorts with study-specific follow-up ranging from 7 to 28 years.
Setting: Academic research.
Patients: Participants in the Nurses' Health Study, the Health Professionals Follow-up Study, the Cancer Prevention Study II Nutrition Cohort, the Multiethnic Cohort, and the National Institutes of Health-AARP (formerly known as the American Association of Retired Persons) Diet and Health Study.
Main outcome measures: Amyotrophic lateral sclerosis deaths identified through the National Death Index. In the Nurses' Health Study and the Health Professionals Follow-up Study, confirmed nonfatal incident ALS was also included.
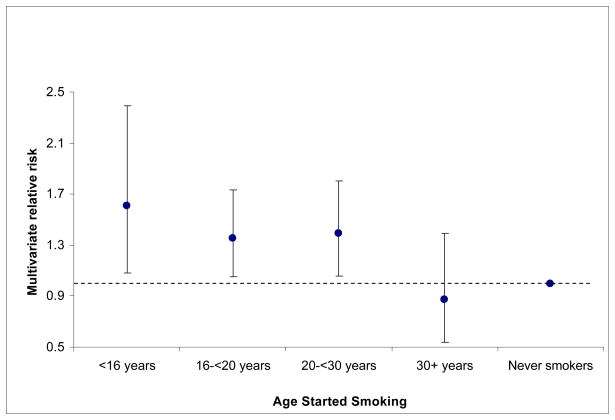
Results: A total of 832 participants with ALS were documented among 562,804 men and 556,276 women. Smokers had a higher risk of ALS than never smokers, with age- and sex-adjusted relative risks of 1.44 (95% confidence interval, 1.23-1.68; P < .001) for former smokers and 1.42 (95% confidence interval, 1.07-1.88; P = .02) for current smokers. Although the risk of ALS was positively associated with pack-years smoked (P < .001), duration of smoking (9% increase for each 10 years of smoking, P = .006), and the number of cigarettes smoked per day (10% increase for each increment of 10 cigarettes smoked per day, P < .001), these associations did not persist when never smokers were excluded. However, among ever smokers, the risk of ALS increased as age at smoking initiation decreased (P = .03).
Conclusions: Results of this large longitudinal study support the hypothesis that cigarette smoking increases the risk of ALS. The potential importance of age at smoking initiation and the lack of a dose response deserve further investigation.
Conflict of interest statement
The authors have no competing interest or financial disclosures.
Figures



References
-
- Walling AD. Amyotrophic lateral sclerosis: Lou Gehrig’s disease. Am Fam Physician. 1999;59:1489–1496. - PubMed
-
- del Aguila MA, Longstreth WT, Jr, McGuire V, et al. Prognosis in amyotrophic lateral sclerosis: a population-based study. Neurology. 2003;60:813–819. - PubMed
-
- Gorelick PBAM, editor. Handbook of neuroepidemiology. New York: Dekker; 1994. pp. 407–456.
-
- Kamel F, Umbach DM, Munsat TL, et al. Association of cigarette smoking with amyotrophic lateral sclerosis. Neuroepidemiology. 1999;18:194–202. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
