

Diagnosis and treatment of common forms of tremor
- PMID: 21321834
- PMCID: PMC3907068
- DOI: 10.1055/s-0031-1271312
Diagnosis and treatment of common forms of tremor
Abstract
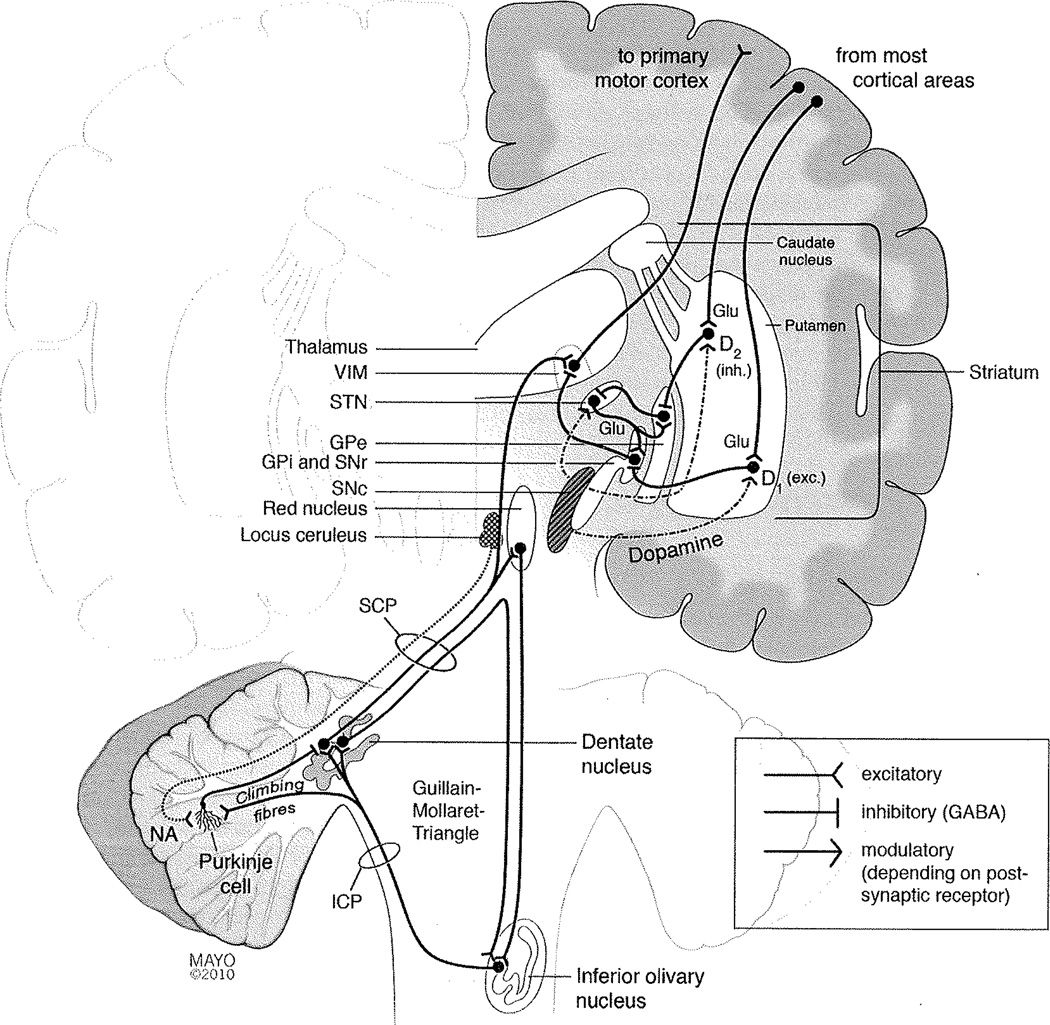
Tremor is the most common movement disorder presenting to an outpatient neurology practice and is defined as a rhythmical, involuntary oscillatory movement of a body part. The authors review the clinical examination, classification, and diagnosis of tremor. The pathophysiology of the more common forms of tremor is outlined, and treatment options are discussed. Essential tremor is characterized primarily by postural and action tremors, may be a neurodegenerative disorder with pathologic changes in the cerebellum, and can be treated with a wide range of pharmacologic and nonpharmacologic methods. Tremor at rest is typical for Parkinson's disease, but may arise independently of a dopaminergic deficit. Enhanced physiologic tremor, intention tremor, and dystonic tremor are discussed. Further differential diagnoses described in this review include drug- or toxin-induced tremor, neuropathic tremor, psychogenic tremor, orthostatic tremor, palatal tremor, tremor in Wilson's disease, and tremor secondary to cerebral lesions, such as Holmes' tremor (midbrain tremor). An individualized approach to treatment of tremor patients is important, taking into account the degree of disability, including social embarrassment, which the tremor causes in the patient's life.
© Thieme Medical Publishers.
Figures
References
-
- Deuschl G, Bain P, Brin M Ad Hoc Scientific Committee. Consensus statement of the Movement Disorder Society on Tremor. Mov Disord. 1998;13(Suppl 3):2–23. - PubMed
-
- Zesiewicz TA, Hauser RA. Phenomenology and treatment of tremor disorders. Neurol Clin. 2001;19(3):651–680. vii vii. - PubMed
-
- Thanvi B, Lo N, Robinson T. Essential tremor-the most common movement disorder in older people. Age Ageing. 2006;35(4):344–349. - PubMed
-
- Louis ED. Essential tremor: evolving clinicopathological concepts in an era of intensive post-mortem enquiry. Lancet Neurol. 2010;9(6):613–622. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
