

Quantitative volumetric analysis of conventional MRI response in recurrent glioblastoma treated with bevacizumab
- PMID: 21324937
- PMCID: PMC3064698
- DOI: 10.1093/neuonc/noq206
Quantitative volumetric analysis of conventional MRI response in recurrent glioblastoma treated with bevacizumab
Abstract
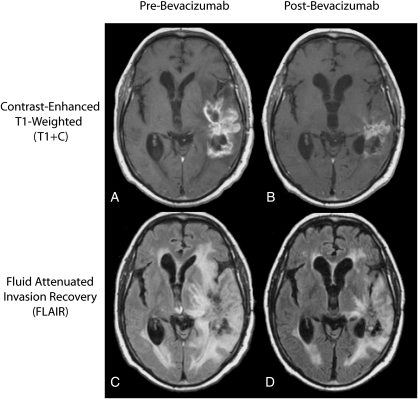
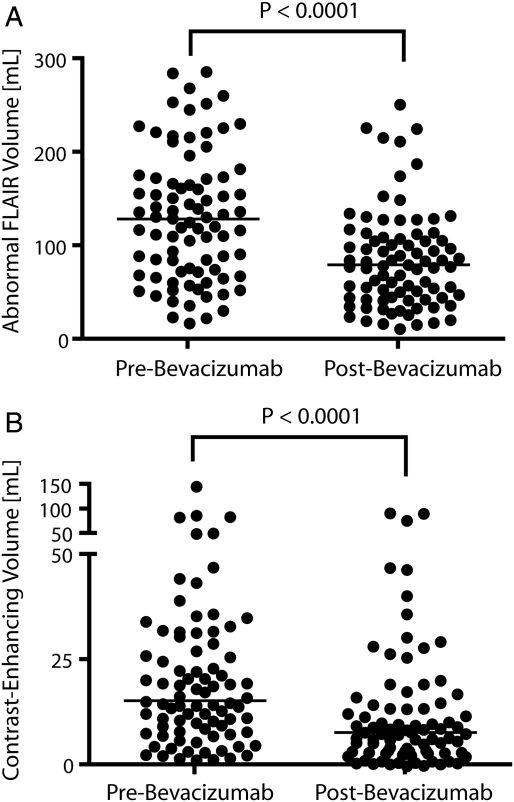
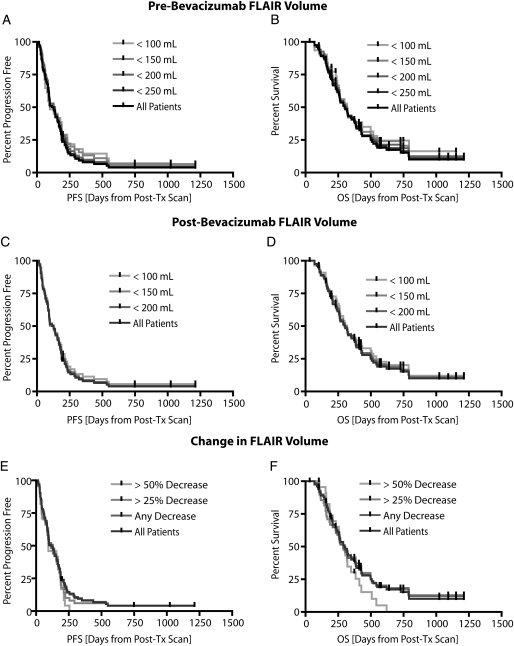
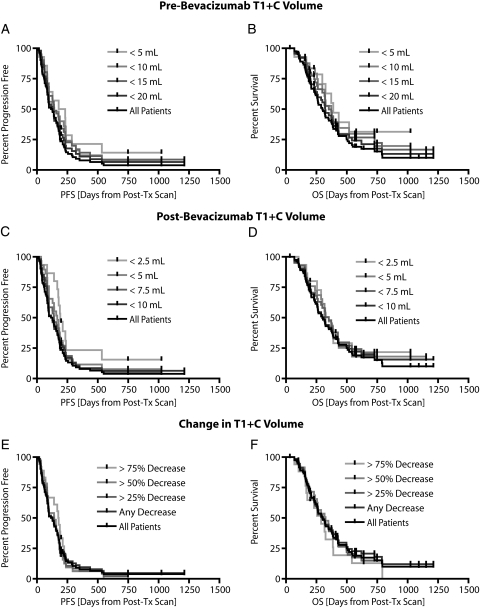
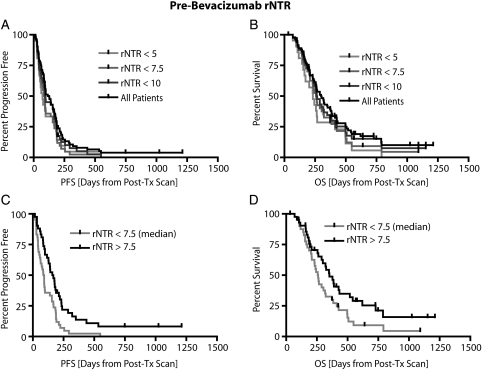
Although the effects of bevacizumab on magnetic resonance images (MRIs) of recurrent glioblastoma multiforme (GBM) are well documented, to our knowledge, no studies have explicitly quantified the volumetric changes resulting from initial treatment, nor have there been studies examining the ability for volumetric changes in conventional MRI to predict progression-free survival (PFS) and overall survival (OS). In the current study, we retrospectively examined volumetric changes on conventional MRI scans in 84 patients with recurrent GBM. MRIs were obtained before (mean, 11 days) and after (mean, 42 days) treatment with bevacizumab. The volume of abnormal fluid-attenuated inversion recovery (FLAIR) signal intensity, the volume of contrast enhancement, and the ratio of the 2 were quantified for each patient before and after initial treatment. Results demonstrated that initial treatment with bevacizumab resulted in a significant decrease in both the volume of abnormal FLAIR signal and the volume of contrast enhancement. Initial, residual, and change in FLAIR volume were not predictive of PFS or OS. Initial contrast-enhancing volume was predictive of PFS but not OS. The pretreatment relative nonenhancing tumor ratio, defined as the ratio of FLAIR to contrast-enhancing volume, was found to be predictive of both PFS and OS.
Figures
References
-
- Plate KH, Breier G, Risau W. Molecular mechanisms of developmental and tumor angiogenesis. Brain Pathol. 1994;4(3):207–218. - PubMed
-
- Holash J, Maisonpierre PC, Compton D, et al. Vessel cooption, regression, and growth in tumors mediated by angiopoietins and VEGF. Science. 1999;284(5422):1994–1998. - PubMed
-
- Vredenburgh JJ, Desjardins A, Herndon JE, et al. Phase II trial of bevacizumab and irinotecan in recurrent malignant glioma. Clin Cancer Res. 2007;13(1253–9) - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
