

Adherence therapy for medication non-compliant patients with hypertension: a randomised controlled trial
- PMID: 21326328
- PMCID: PMC3257548
- DOI: 10.1038/jhh.2010.133
Adherence therapy for medication non-compliant patients with hypertension: a randomised controlled trial
Abstract
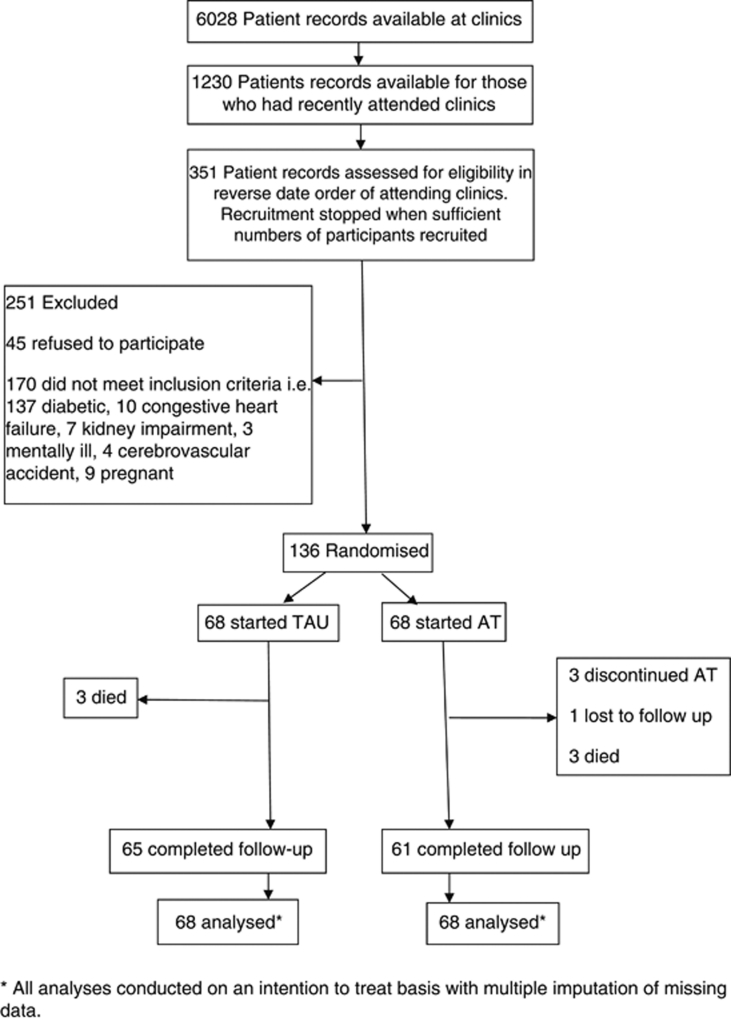
The objective of this study is to establish the efficacy of adherence therapy (AT) compared with treatment as usual (TAU) in reducing blood pressure (BP) in non-compliant hypertensive patients. This study was designed as a parallel-group single-blind randomised controlled trial. The study was carried out at three general hospital outpatient clinics in Jordan. A total of 136 non-compliant hypertensive patients with a mean baseline BP of 164.5 mm Hg (s.d. 10.0) over 102.2 mm Hg (s.d. 7.0) participated in the study. 7 weekly 20-min sessions of AT in addition to TAU. The main outcome of this study is systolic blood pressure (SBP) at 11-weeks follow-up. In all, 68 patients received TAU and 68 AT. Intention-to-treat analysis included all participants randomised. AT lowered SBP by -23.11 mm Hg (95% CI: -25.85, -20.36) and diastolic BP (DBP) by -15.18 mm Hg (95% CI: -17.55, -12.80) at 11 weeks compared with TAU. Adherence (measured by pill counting) was also improved in the AT group by 37% at 11 weeks compared with TAU. No significant adverse events were reported. AT increases adherence to medication for hypertension which then leads to a clinically important reduction in BP.
Figures
References
-
- World Health Organization, International Society of Hypertension Writing Group World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J Hypertens. 2003;21:1983–1992. - PubMed
-
- Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. The Lancet. 2005;365:217–223. - PubMed
-
- Ezzati M, Lopez A, Rodgers A, Vander Hoorn S, Murray C. Selected major risk factors and global and regional burden of disease. Lancet. 2002;360:1347–1360. - PubMed
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. The Lancet. 2002;360:1903–1913. - PubMed
-
- MacMahon S, Peto R, Collins R, Godwin J, Cutler J, Sorlie P, et al. Blood pressure, stroke, and coronary heart disease: Part 1, prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. The Lancet. 1990;335:765–774. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
