

doi: 10.1055/s-0028-1085924.
Visceral trauma: principles of management and role of embolotherapy
Affiliations
- PMID: 21326517
- PMCID: PMC3036445
- DOI: 10.1055/s-0028-1085924
Item in Clipboard
Visceral trauma: principles of management and role of embolotherapy
Semin Intervent Radiol.
2008 Sep.
Abstract
Interventional radiology for the treatment of traumatic visceral hemorrhage has emerged as an important adjunct to modern trauma care. This article outlines the general surgical concepts of the acute care of trauma patients as a guideline for catheter-based therapy. Specific considerations are presented for embolizing visceral injuries in the liver, spleen, and kidney. Expected outcomes and follow-up are reviewed.
Keywords: Trauma; damage control laparotomy; hepatic embolization; hepatic hemorrhage; renal embolization; splenic embolization.
Figures
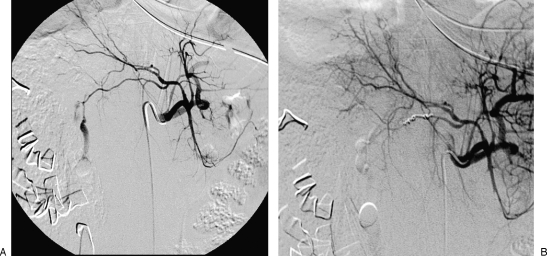
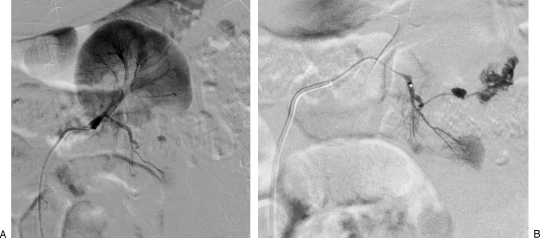
(A) Initial anteroposterior celiac angiogram on a young trauma patient following high-speed motor vehicle crash. The patient had continuing arterial bleeding despite damage control laparotomy and packing. A vigorous bleed is seen originating from a right hepatic artery branch. (B) Completion celiac angiogram on the patient following subselective catheterization and embolization shows achieved hemostasis.
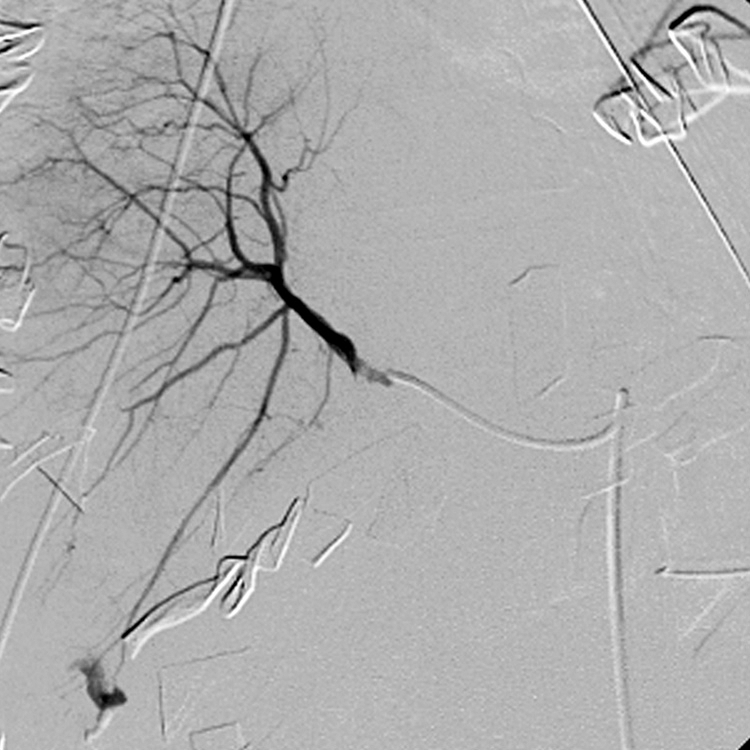
Right hepatic angiogram in a patient with continuous bleeding following hepatic packing. Active arterial bleeding is noted adjacent to the surgical pack.
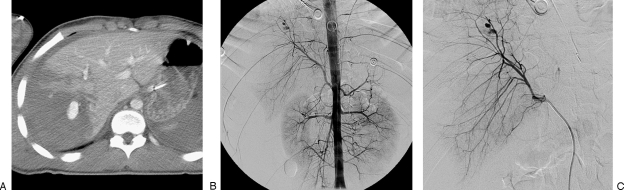
(A) Abdominal computed tomography in a trauma patient following 30-foot fall. There is extensive liver laceration and focal pseudoaneurysm. (B) Abdominal aortogram confirms active bleeding and conventional anatomy. (C) Selective right hepatic angiogram was performed before microcatheter selection and embolization.
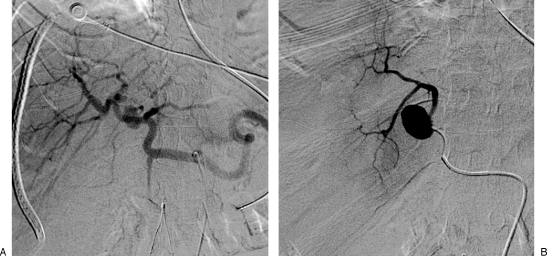
A 44-year-old man after crush injury and grade 3 liver laceration resulting in hemobilia. (A) Celiac angiogram demonstrates a 2-cm pseudoaneurysm arising from a small early branch of the right hepatic artery. (B) Angiogram with microcatheter in the pseudoaneurysm showing an outflow vessel. The distal vessel could not be catheterized and thus large particles, 900 to 1100 μm, were slowly delivered to block potential backbleeding. The pseudoaneurysm and inflow branch were then coil embolized.

Celiac angiogram demonstrates a traumatic pseudoaneurysm arising from between the left and right hepatic arteries. Selective catheterization is necessary to further diagnose and treat the focal bleed.
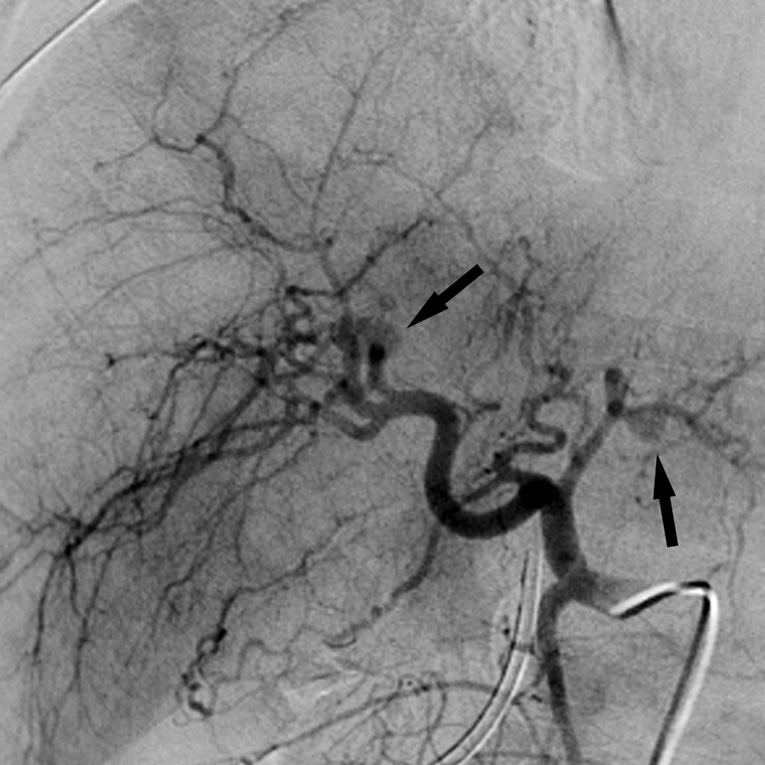
Common hepatic angiogram shows two pseudoaneurysms (black arrows) in this trauma patient after high-speed motor vehicle crash. Note variant middle hepatic branch. Treating multiple hepatic targets is difficult because the left and right hepatic arteries require subselective embolization to preserve organ function.
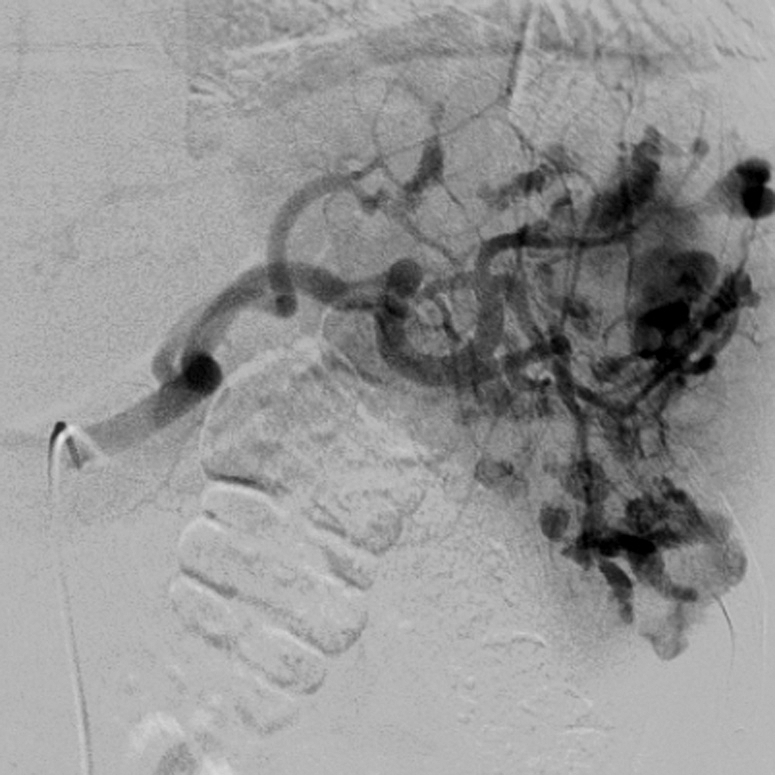
Splenic angiogram shows multiple pseudoaneurysms.
Splenic angiogram shows innumerable small pseudoaneurysms, too numerous to embolize individually. Proximal coil embolization was performed.
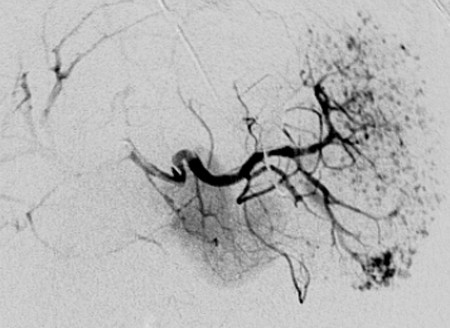
Splenic angiogram after proximal coil embolization shows reconstitution of the distal splenic artery via the dorsal pancreatic to the transverse pancreatic to the pancreaticomagna collateral route. This allows healing of the injury without inducing infarction of the spleen.

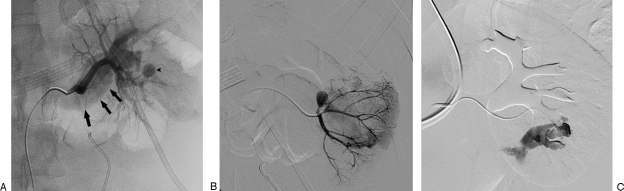
Penetrating trauma to the left flank and hematuria prompted angiographic evaluation. (A) Aortogram shows normal renal artery anatomy and a small inferior pole bleed. (B) Selective left renal angiogram demonstrates the bleed to arise from an interlobar branch. (C) Final angiogram following coil embolization demonstrates cessation of hemorrhage.
(A) Left renal angiogram in a patient with an accessory lower pole artery. Note lack of parenchymal enhancement of the lower pole when studying the upper pole artery. (B) Microcatheter selective angiogram shows active bleeding originating from an arcuate branch. This was selectively coil embolized from this position.
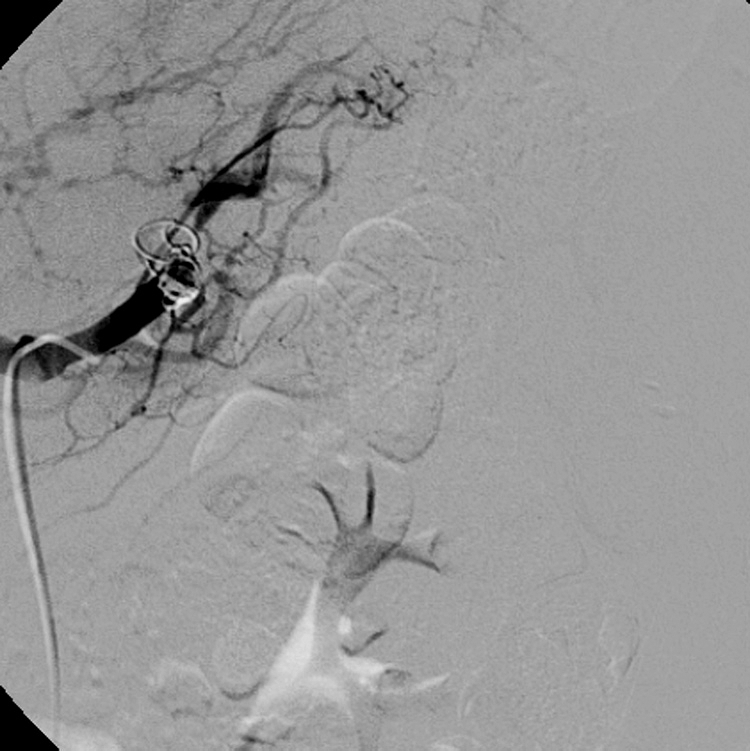
(A) Left renal angiogram in this young patient with intermittent large-volume hematuria 1 week after penetrating trauma to the left flank. A pseudoaneurysm with early filling of the renal vein (arrows) was discovered. (B) Selective angiogram on the same patient demonstrates the aneurysm. (C) Catheter is seen positioned through the pseudoaneurysm into a portion of the fistula and renal vein. This complex lesion was treated with coil embolization, which resolved the hematuria.
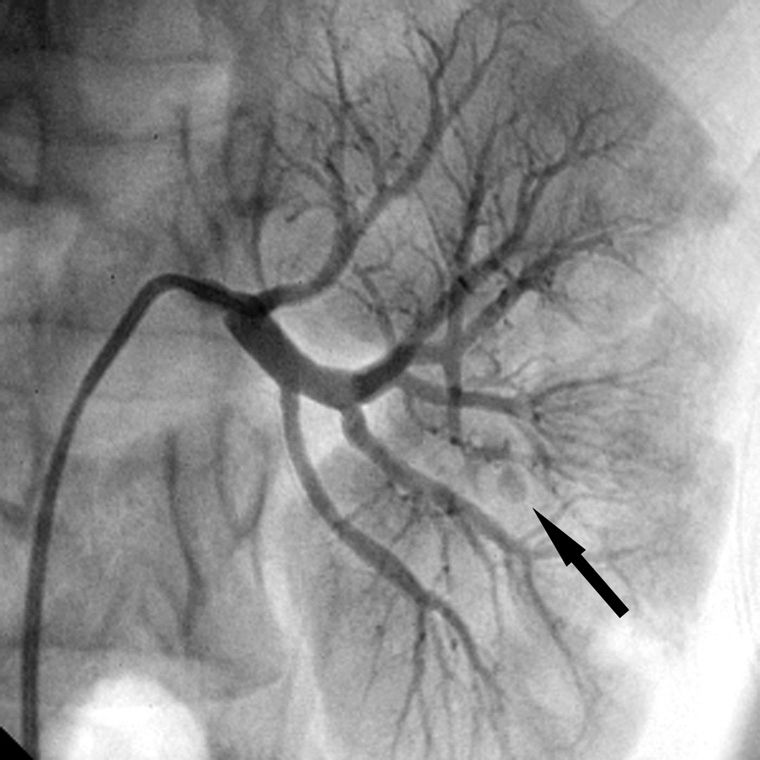
Selective left renal angiogram shows a subtle pseudoaneurysm (arrow).
Similar articles
-
Interventional Radiology service provision and practice for the management of traumatic splenic injury across the Regional Trauma Networks of England.Injury. 2017 May;48(5):1031-1034. doi: 10.1016/j.injury.2017.02.031. Epub 2017 Feb 27. Injury. 2017. PMID: 28292519
-
Managing penetrating renal trauma: experience from two major trauma centres in the UK.BJU Int. 2018 Jun;121(6):928-934. doi: 10.1111/bju.14165. Epub 2018 Mar 13. BJU Int. 2018. PMID: 29438587
-
Interventional Radiology in Renal Trauma.Semin Intervent Radiol. 2021 Mar;38(1):113-122. doi: 10.1055/s-0041-1726006. Epub 2021 Apr 15. Semin Intervent Radiol. 2021. PMID: 33883808 Free PMC article. Review.
-
Surgical intervention for paediatric liver injuries is almost history - a 12-year cohort from a major Scandinavian trauma centre.Scand J Trauma Resusc Emerg Med. 2016 Nov 29;24(1):139. doi: 10.1186/s13049-016-0329-x. Scand J Trauma Resusc Emerg Med. 2016. PMID: 27899118 Free PMC article.
-
Non-operative management of hepatic trauma and the interventional radiology: an update review.Indian J Surg. 2013 Oct;75(5):339-45. doi: 10.1007/s12262-012-0712-4. Epub 2012 Aug 3. Indian J Surg. 2013. PMID: 24426473 Free PMC article. Review.
Cited by
-
Renal embolization for trauma: a narrative review.J Trauma Inj. 2024 Sep;37(3):171-181. doi: 10.20408/jti.2024.0021. Epub 2024 Sep 24. J Trauma Inj. 2024. PMID: 39428726 Free PMC article.
-
Celiac trunk arterial variations and their clinical implications: Role of imaging.Indian J Gastroenterol. 2024 Dec;43(6):1099-1110. doi: 10.1007/s12664-024-01656-5. Epub 2024 Sep 7. Indian J Gastroenterol. 2024. PMID: 39243342 Review.
-
Endovascular intervention in renovascular disease: a pictorial review.Insights Imaging. 2014 Dec;5(6):667-76. doi: 10.1007/s13244-014-0363-z. Epub 2014 Oct 12. Insights Imaging. 2014. PMID: 25304038 Free PMC article.
References
-
- Feliciano D V, Mattox D L, Moore E E. Trauma. 6th ed. San Francisco: McGraw-Hill; 2008. p. 1430.
-
- Kashuk J L, Moore E E, Millikan J S, Moore J B. Major abdominal vascular trauma–a unified approach. J Trauma. 1982;22(8):672–679. - PubMed
-
- Johnson J W, Gracias V H, Schwab C W, et al. Evolution in damage control for exsanguinating penetrating abdominal injury. J Trauma. 2001;51(2):261–269. discussion 269–271. - PubMed
-
- Parr M J, Alabdi T. Damage control surgery and intensive care. Injury. 2004;35(7):713–722. - PubMed
-
- Department of Defense Surface ship survivability. Naval War Publication 3-20.31. Washington, DC: U.S. Government Printing Office; 1996.
