

Mesenteric vasculature and collateral pathways
- PMID: 21326561
- PMCID: PMC3036491
- DOI: 10.1055/s-0029-1225663
Mesenteric vasculature and collateral pathways
Abstract
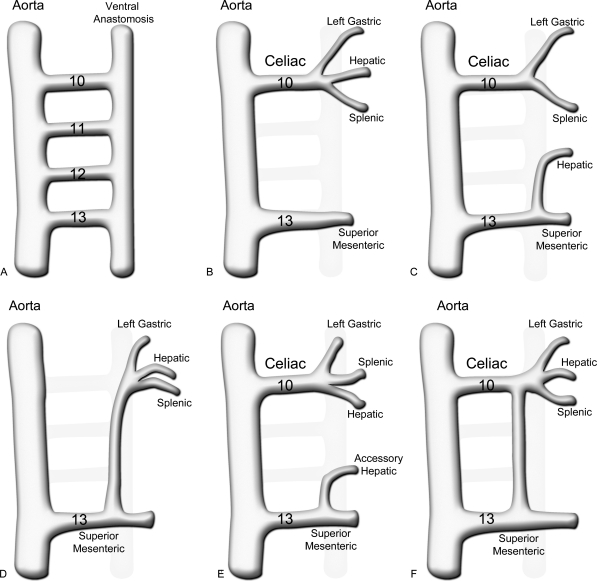
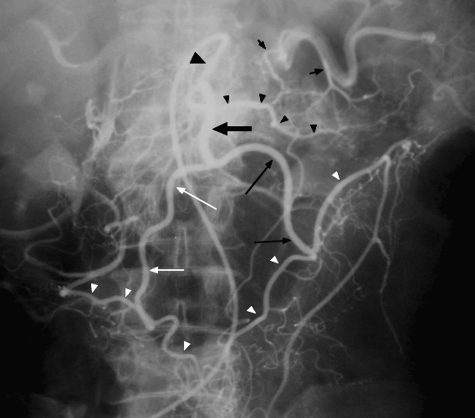
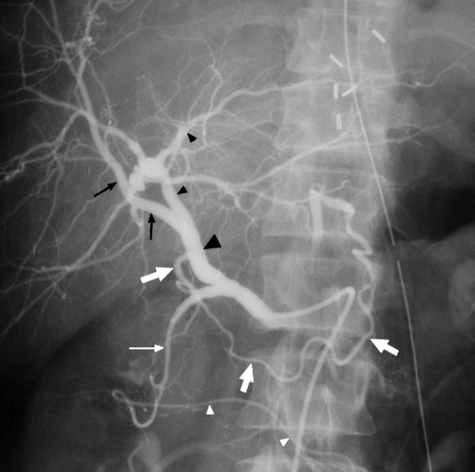
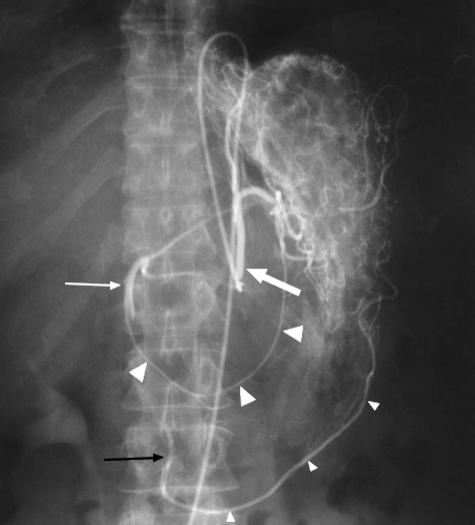
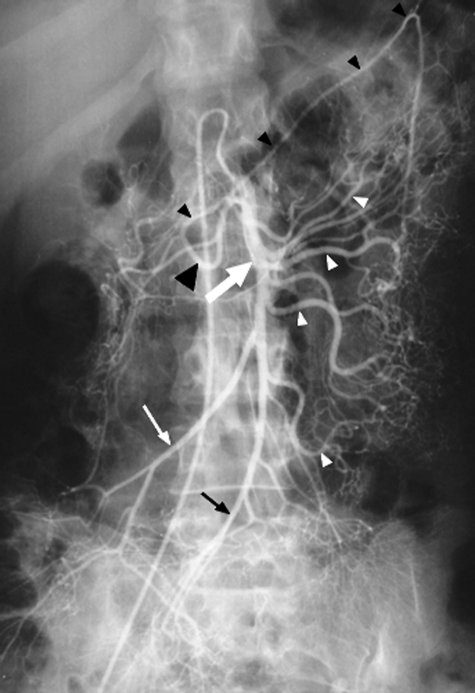
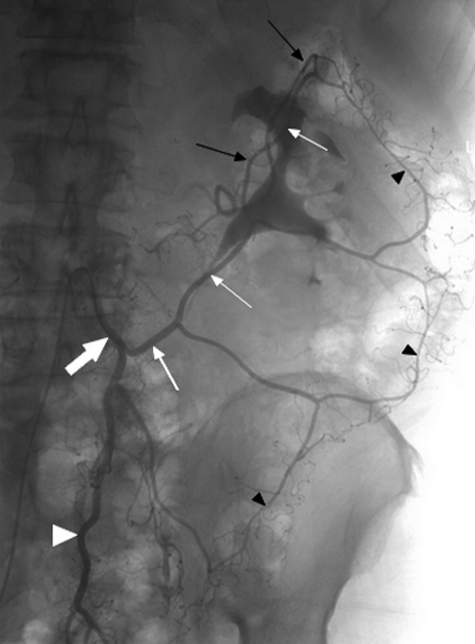
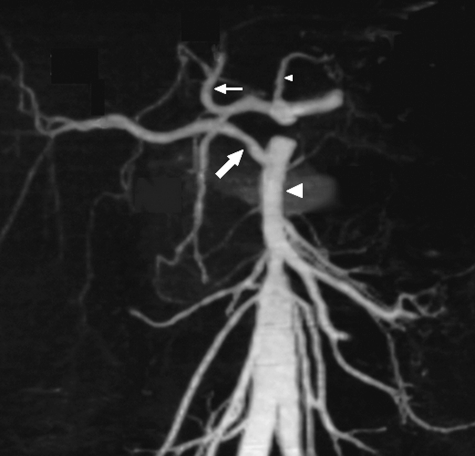
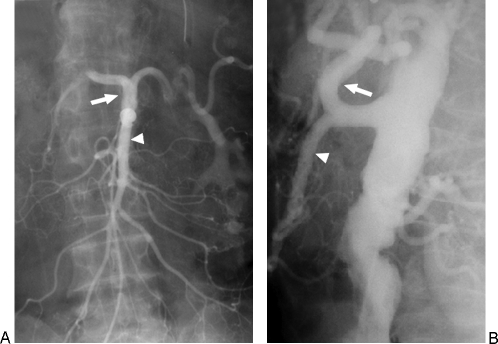
The arterial and venous circulation of the bowel is complex and is characterized by marked redundancy of multiple interconnecting branches, which provides a rich blood supply to aid in the digestive process and also serves to protect the bowel from potential ischemia or infarction. As a result of this circulatory pattern, anatomic variants and extensive collateral pathways are common. A thorough knowledge of both the arterial and venous mesenteric circulation, including normal, variant, and collateral anatomy, is necessary for the appropriate evaluation and management of the various disease processes that may affect the vascular supply of the gastrointestinal system.
Keywords: Mesenteric circulation; mesenteric collateral pathways; variant arterial anatomy.
Figures



References
-
- Reuter S R, Redman H C, Cho K J. Gastrointestinal Angiography. 3rd ed. Philadelphia, PA: WB Saunders; 1986.
-
- Kaufman J A, Lee M J. Vascular and Interventional Radiology: The Requisites. St. Louis, MO: Mosby; 2004.
-
- Petscavage J M, Maldjian P. Celiomesenteric trunk: two variants of a rare anomaly. Australas Radiol. 2007;51(Suppl):B306–B309. - PubMed
-
- Iezzi R, Cotroneo A R, Giancristofaro D, Santoro M, Storto M L. Multidetector-row CT angiographic imaging of the celiac trunk: anatomy and normal variants. Surg Radiol Anat. 2008;30(4):303–310. - PubMed
-
- McNulty J G, Hickey N, Khosa F, O'Brien P, O'Callaghan J P. Surgical and radiological significance of variants of Bühler's anastomotic artery: a report of three cases. Surg Radiol Anat. 2001;23(4):277–280. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
