

Catheter-directed thrombolysis for acute limb ischemia
- PMID: 21326772
- PMCID: PMC3036379
- DOI: 10.1055/s-2006-948765
Catheter-directed thrombolysis for acute limb ischemia
Abstract
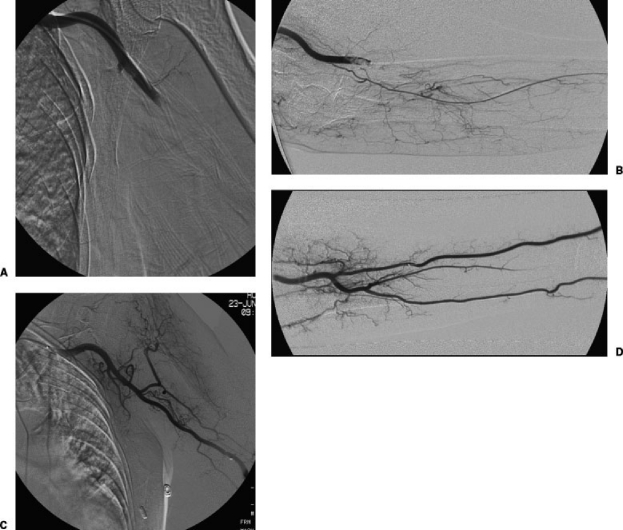
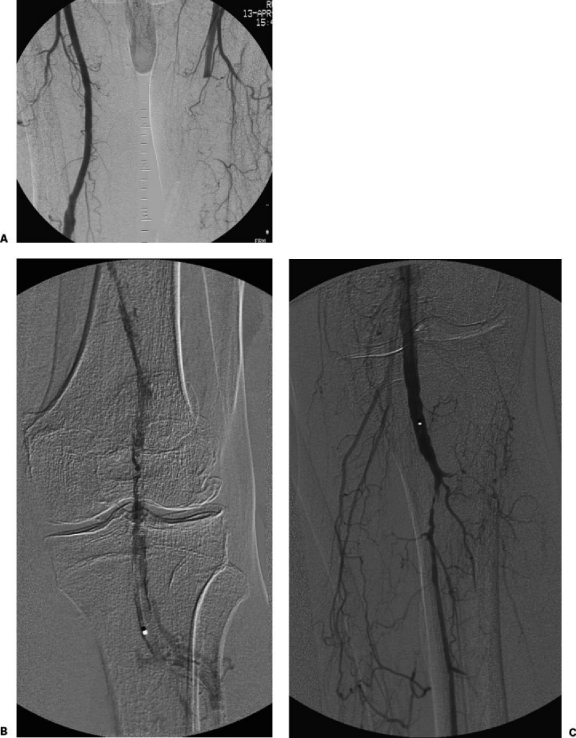
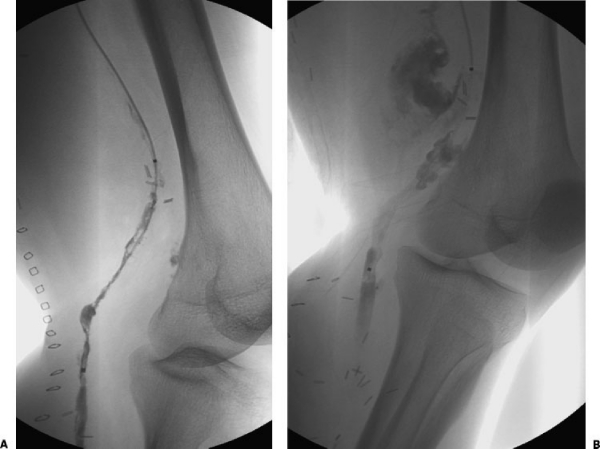
Acute limb ischemia is a potentially life-threatening clinical event. Thrombosis in situ, bypass graft thrombosis, and embolic occlusion are the three major precipitating events leading to acute limb ischemia. Management of acute ischemia depends on the clinical status of the affected limb and patient comorbidities. Catheter-directed thrombolysis (CDT) is the treatment of choice for patients with relatively mild acute limb ischemia (Rutherford categories I and IIa) with no contraindications to thrombolytic therapy. Patients with severe acute limb ischemia (Rutherford category IIb) need emergent revascularization. CDT should be considered, nonetheless, if the relative risks compared with primary operation are favorable. CDT is a life- and limb-saving treatment for many patients despite limitations of efficacy and associated complications. This article is a review of the etiology of acute arterial occlusion; clinical triage of patients presenting with acute limb ischemia; catheter guide wire techniques, pharmacological agents, and devices in current use for CDT; as well as the outcomes of CDT.
Keywords: Thrombolysis; acute limb ischemia; anticoagulation; plasminogen activator.
Figures
References
-
- Kasirajan K, Ouriel K. Management of acute lower extremity ischemia: treatment strategies and outcome. Curr Interv Cardiol Rep. 2000;2:119–129. - PubMed
-
- Camerta A, White J V. In: Camerta A, editor. Thrombolytic Therapy for Peripheral Vascular Disease. Philadelphia: Lippincott-Ravenm; 1995. Overview of catheter directed thrombolytic therapy for arterial and graft occlusion. pp. 249–252.
-
- Dotter C T, Rosch J, Seaman A J. Selective clot lysis with low-dose streptokinase. Radiology. 1974;111:31–37. - PubMed
-
- Kasirajan K, Haskal Z J, Ouriel K. The use of mechanical thrombectomy devices in the management of acute peripheral arterial occlusive disease. J Vasc Interv Radiol. 2001;12:405–411. - PubMed
-
- Hirsch A T, Haskal Z J, Hertzer N R, et al. ACC/AHA Guidelines for the Management of Patients with Peripheral Arterial Disease (Lower Extremity, Renal, Mesenteric, and Abdominal Aortic): A Collaborative Report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society for Vascular Medicine and Biology, and the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients with Peripheral Arterial Disease). American College of Cardiology Web Site. Available at: http://www.acc.orglclinicaJ/guidelines/padlindex.pdf. Accessed March 16, 2006. Available at: http://www.acc.orglclinicaJ/guidelines/padlindex.pdf - PubMed
