

doi: 10.1055/s-2007-980040.
Aortic development and anomalies
Affiliations
- PMID: 21326792
- PMCID: PMC3036416
- DOI: 10.1055/s-2007-980040
Item in Clipboard
Aortic development and anomalies
Semin Intervent Radiol.
2007 Jun.
Abstract
Development of the aorta takes place during the third week of gestation. It is a complex process that can lead to a variety of congenital variants and pathological anomalies. In diagnostic and interventional radiology, knowledge of aortic abnormalities and variant branching sequence is crucially important. This article gives a systematic overview of anatomical variability of the aorta.
Keywords: Thoracic aorta; anatomical variants; embryology.
Figures
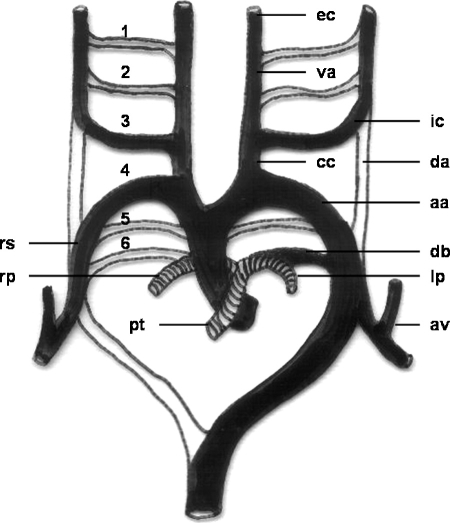
Schematic drawing of the development of the aortic arch and its branches. 1, first aortic arch; 2, second aortic arch; 3, third aortic arch; 4, fourth aortic arch; 5, fifth aortic arch; 6, sixth aortic arch; aa, aortic arch; va, ventral aorta; da, dorsal aorta; cc, common carotid artery; ic, internal carotid artery; ec, external carotid artery; rs, right subclavian artery; av, vertebral artery; pt, pulmonary trunk; rp, right pulmonary artery; lp, left pulmonary artery; db, ductus arteriosus Botalli.
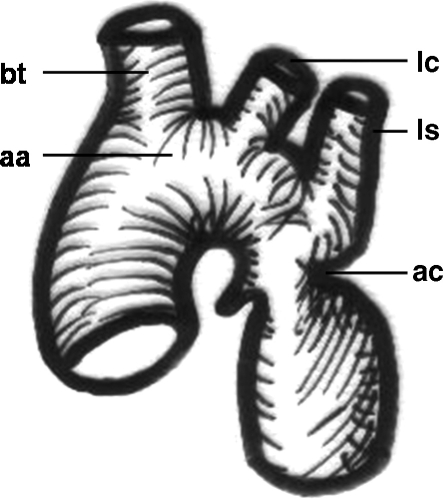
Schematic drawing of an aortic coarctation. aa, aortic arch; bt, brachiocephalic trunk; lc, left carotid artery; ls, left subclavian artery; ac, coarctation of the aorta.
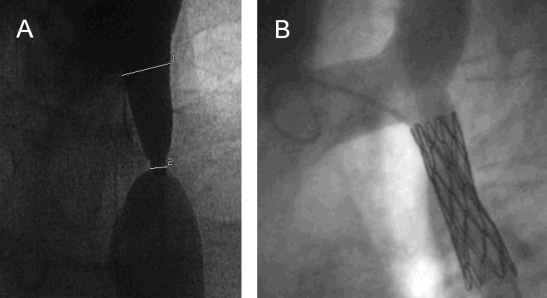
Angiogram in a 35-year-old patient showing (A) postductal coarctation of the aorta with upstream segmental hypoplasia. (B) Stenting reduced the systolic blood pressure gradient from 50 mm Hg to below 20 mm Hg. (Images courtesy of A. Gamillscheg, Department of Pediatric Cardiology, Medical University of Graz, Graz, Austria.)
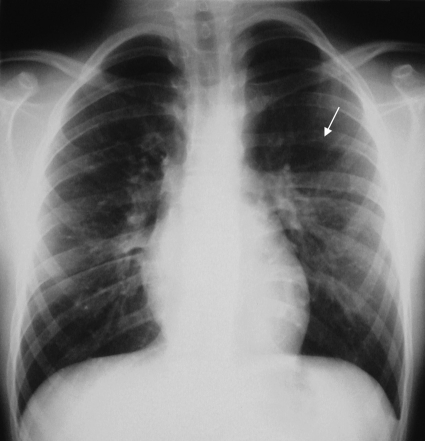
Plain chest radiograph in a 12-year-old boy with proven coarctation of the aorta. Rib notching (arrow) due to pressure erosion indicates enlargement and tortuosity of intercostal arteries that provide collateral blood flow to circumvent the stenotic aortic segment.
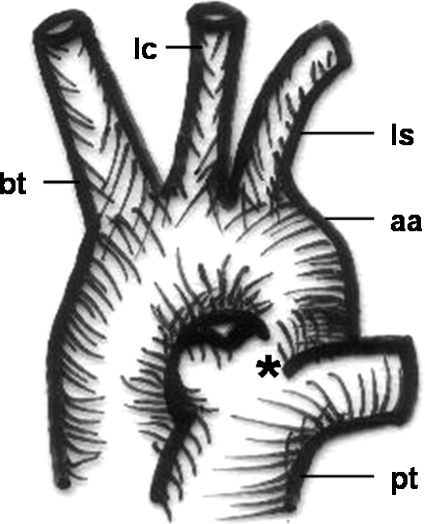
Schematic drawing of a patent ductus arteriosus Botalli. bt, brachiocephalic trunk; lc, left carotid artery; ls, left subclavian artery; aa, aortic arch; pt, pulmonary trunk; *, ductus arteriosus.
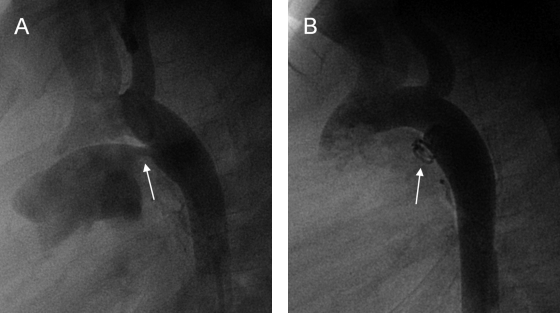
(A) Aortogram (lateral view) depicting a patent ductus arteriosus (arrow). (B) Repeat angiogram showing endovascular coiling (arrow) was successful in this young adult patient. (Images courtesy of A. Gamillscheg, Department of Pediatric Cardiology, Medical University of Graz, Graz, Austria.)
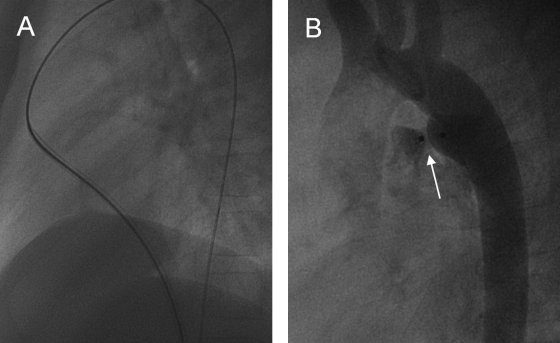
Occlusion of a patent ductus arteriosus in an adolescent with the use of Amplatzer (AGA, Golden Valley, MN) duct occluder. (A) During this intervention fluoroscopic images show the sheath (here with guidewire) taking the following course: inferior vena cava—right atrium—right ventricle—pulmonary trunk—patent ductus arteriosus—descending aorta. (B) Postintervention aortography shows minor residual shunt. (Images courtesy of A. Gamillscheg, Department of Pediatric Cardiology, Medical University of Graz, Graz, Austria.)
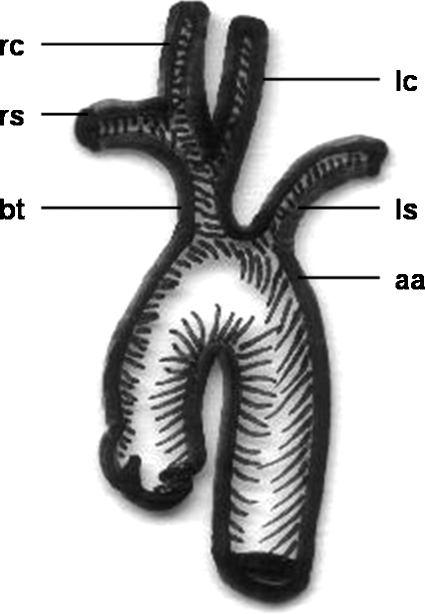
Schematic drawing of a “bovine trunk.” rc, right carotid artery, rs, right subclavian artery; bt, “bovine trunk” (common trunk of right subclavian and both carotid arteries); lc, left carotid artery; ls, left subclavian artery; aa, aortic arch.
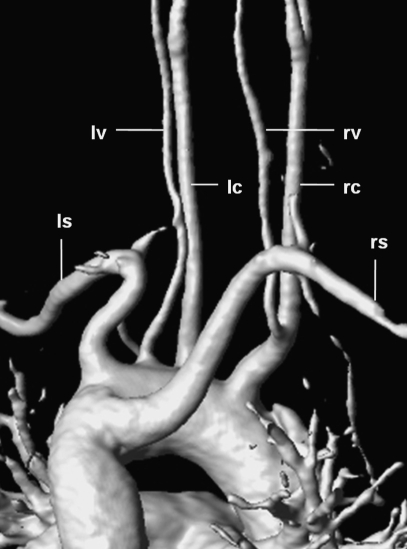
3D-reconstructed magnetic resonance angiography in a 38-year-old woman showing a rare branching pattern of the aortic arch (view from posterior). The right common carotid artery (rc) gives rise to the right vertebral artery (rv); the left vertebral artery (lv) arises directly from the aortic arch between the left common carotid artery (lc) and the left subclavian artery (ls); the right subclavian artery (rs) originates as the last branch and takes a retroesophageal course (“arteria lusoria”).
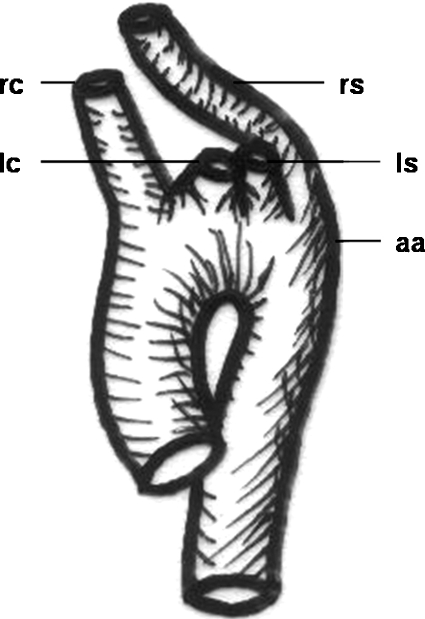
Schematic drawing of a variant branching sequence of supra-aortal arteries with the right subclavian artery originating distal to the left one. rc, right carotid artery; lc, left carotid artery; ls, left subclavian artery; rs, right subclavian artery; aa, aortic arch.

Image of a barium swallow test in a 6-year-old boy showing a suggestive posterior notch of the esophagus (arrow). “Arteria lusoria” (retroesophageal course of the right subclavian artery) has been confirmed by computed tomography (not shown).

Plain chest radiograph in a 7-year-old boy depicting a right aortic arch (arrow). Absence of a left-sided aortic knob is the even more apparent sign.
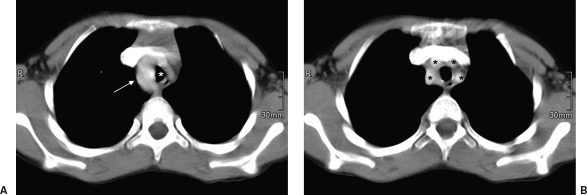
(A) Contrast-enhanced computed tomography in a 7-year-old boy with a right aortic arch (arrow) narrowing the trachea (white asterisk). (B) As another variation, the four supra-aortal arteries (black asterisks) originate separately.
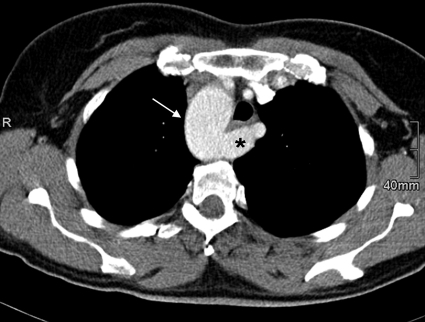
Contrast-enhanced computed tomography in a 42-year-old woman with a right aortic arch (arrow) showing the pattern of a so-called arteria pseudolusoria. The left subclavian artery (asterisk) is crossing posterior to the esophagus and trachea.
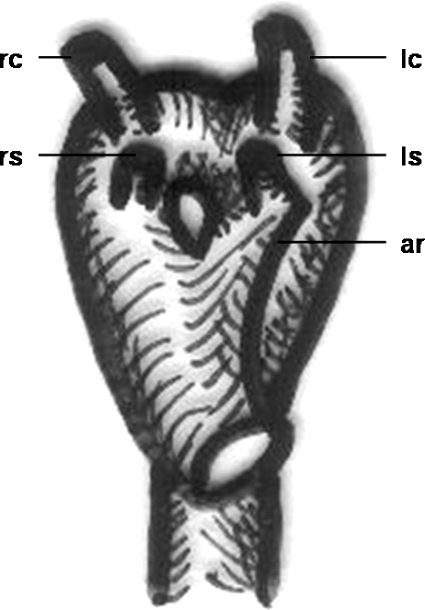
Schematic drawing of a double aortic arch with aortic ring formation. rs, right subclavian artery; rc, right carotid artery; lc, left carotid artery; ls, left subclavian artery; ar, aortic ring.
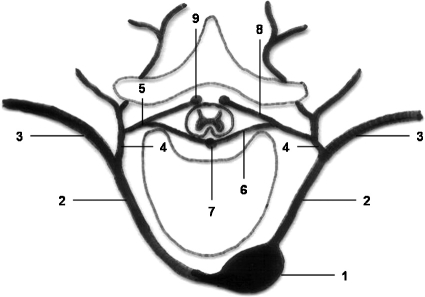
Schematic drawing of the posterior intercostal artery and its dorsal branch. 1, thoracic aorta; 2, posterior intercostal artery; 3, ventral branch; 4, dorsal branch; 5, spinal branch; 6, anterior radicular branch; 7, anterior spinal artery; 8, posterior radicular branch; 9, posterior spinal artery. (Modified from Leonhardt.34)
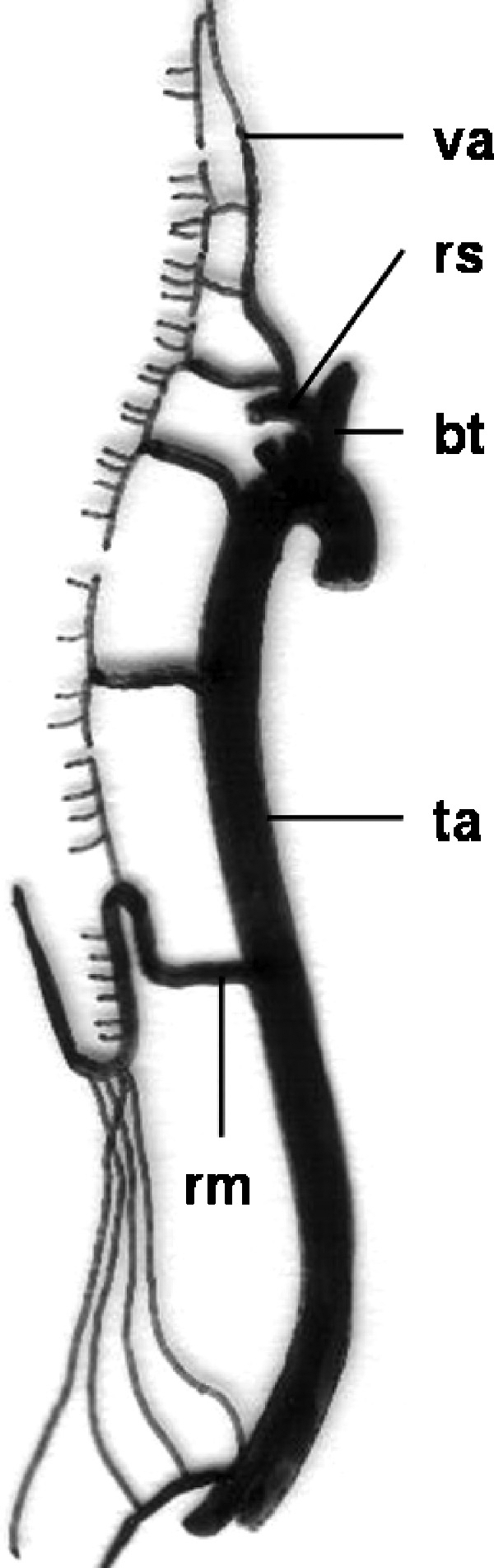
Schematic drawing of blood supply of the spinal cord. va, vertebral artery; rs, right subclavian artery; bt, brachiocephalic trunk; ta, thoracic aorta; rm, arteria radicularis magna (Adamkiewicz). (Modified from Leonhardt.34)

Angiography in a 27-year-old patient presenting with recurrent hemoptysis shows anomalous systemic arterial supply to the posterobasal segment of the right lower pulmonary lobe. (A) The feeding artery (arrow) arises from the celiac trunk. (B) Selective angiography depicts racemose vessels (asterisk) in the lung base and a draining pulmonary vein (arrow). (C) Computed tomography shows the area of “pseudo-sequestration” (long arrow) and the abnormal artery (short arrow). (D) After embolization with microspheres and coiling (arrow) of the feeding artery, the posterobasal segment of the right lower lobe has normalized in computed tomography.
References
-
- Kadir S. In: Kadir S, editor. Atlas of Normal and Variant Angiographic Anatomy. Philadelphia: WB Saunders; 1991. Regional anatomy of the thoracic aorta. pp. 19–54.
-
- Weinberg P M. Aortic arch anomalies. J Cardiovasc Magn Reson. 2006;8:633–643. - PubMed
-
- Bardo D M, Frankel D G, Applegate K E, Murphy D J, Saneto R P. Hypoplastic left heart syndrome. Radiographics. 2001;21:705–717. - PubMed
-
- Devloo-Blancquaert A, Titus J L, Edwards J E, Vallaeys J H, De Gezelle H R, Coppens M. Interruption of aortic arch and hypoplastic left heart syndrome. Pediatr Cardiol. 1995;16:304–308. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
