

Changes in serum-free light chain rather than intact monoclonal immunoglobulin levels predicts outcome following therapy in primary amyloidosis
- PMID: 21328431
- PMCID: PMC3773466
- DOI: 10.1002/ajh.21948
Changes in serum-free light chain rather than intact monoclonal immunoglobulin levels predicts outcome following therapy in primary amyloidosis
Abstract
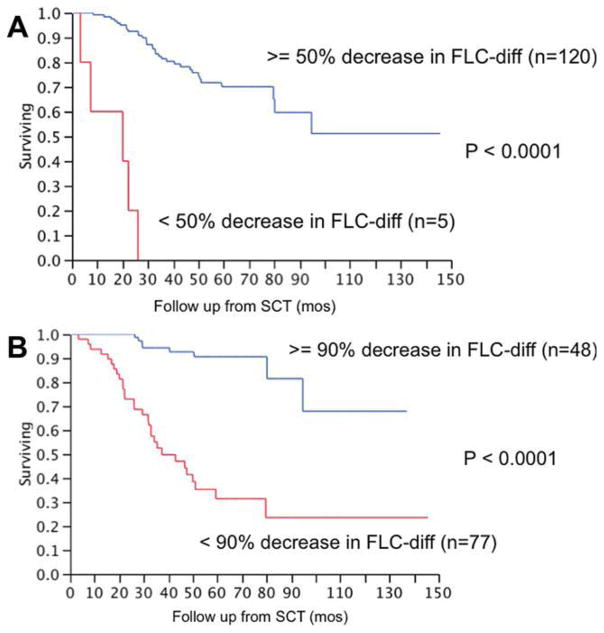
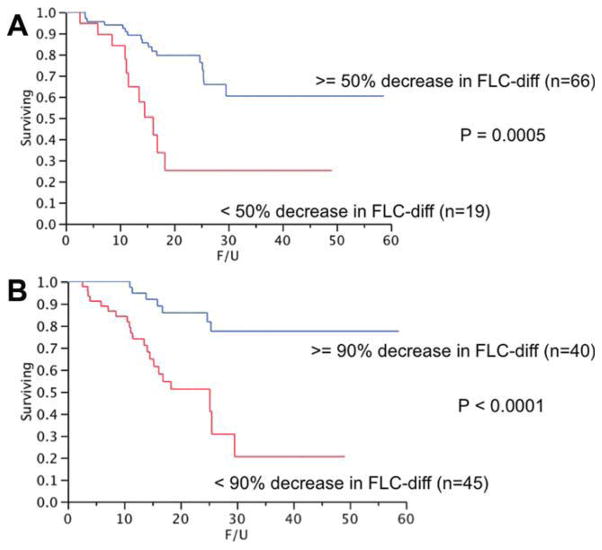
Current response criteria for light-chain amyloidosis (AL) relegate FLC response to a subsidiary status relative to serum M-protein response. Given that light chains form the substrate for amyloid fibril formation, we hypothesized that changes in FLC might better predict outcome compared to changes in intact immunoglobulin levels. Two patient cohorts were studied, 347 patients who underwent an autologous stem-cell transplant (SCT) and 96 patients treated with melphalan/dexamethasone. We identified the lowest value following therapy for intact serum M-protein and the difference between involved and uninvolved FLC (FLC-diff). We first examined the relative contribution of M-protein and FLC-diff on the overall survival (OS), and found that FLC reduction, rather than M-protein reduction, significantly impacted OS. The median OS was not reached among those with a 50% decrease in FLC-diff compared to 20 months for the remainder. On regression analysis, a 90% reduction in FLC-diff following SCT best predicted being alive at 3 or 5 years. The median OS among those with a 90% decrease was not reached compared to 37.4 months for the rest P < 0.001. The current study supports the notion that FLC response is a more useful measure of hematological response than M-protein response. It also highlights the importance of achieving at least a 90% reduction in the FLC-diff to improve the outcome of patients with light-chain AL.
Copyright © 2011 Wiley-Liss, Inc.
Conflict of interest statement
Conflict of interest: SKK was involved in design of concept, data collection, analysis, and writing the paper, AD, MQL, SRH, SRZ, FKB, NL, RAK, SVR, and MAG were involved in writing the manuscript. AD, Honoraria from Binding site for lecture. RAK, Honoraria from Binding site for lecture. SKK, MQL, SRH, SRZ, FKB, NL, SVR, and MAG none relevant to this manuscript.
Figures
References
-
- Kyle RA, Bayrd ED. “Primary” systemic amyloidosis and myeloma. Discussion of relationship and review of 81 cases. Arch Intern Med. 1961;107:344–353. - PubMed
-
- Kyle RA, Gertz MA. Primary systemic amyloidosis: Clinical and laboratory features in 474 cases. Semin Hematol. 1995;32:45–59. - PubMed
-
- Gertz MA, Lacy MQ, Dispenzieri A, Hayman SR. Amyloidosis. Best Pract Res Clin Haematol. 2005;18:709–727. - PubMed
-
- Dispenzieri A, Gertz MA, Kyle RA, et al. Serum cardiac troponins and N-terminal pro-brain natriuretic peptide: A staging system for primary systemic amyloidosis. J Clin Oncol. 2004;22:3751–3757. - PubMed
-
- Gertz MA, Comenzo R, Falk RH, et al. Definition of organ involvement and treatment response in immunoglobulin light chain amyloidosis (AL): A consensus opinion from the 10th International Symposium on Amyloid and Amyloidosis, Tours, France, 18–22 April 2004. Am J Hematol. 2005;79:319–328. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical