

Agility and perturbation training techniques in exercise therapy for reducing pain and improving function in people with knee osteoarthritis: a randomized clinical trial
- PMID: 21330451
- PMCID: PMC3070919
- DOI: 10.2522/ptj.20100188
Agility and perturbation training techniques in exercise therapy for reducing pain and improving function in people with knee osteoarthritis: a randomized clinical trial
Abstract
Background: Impairment-based exercise programs have yielded only small to moderate benefits in reducing pain and improving function in people with knee osteoarthritis (OA). It has previously been proposed that adding agility and perturbation training to exercise programs for people with knee OA may improve treatment effects for pain and function.
Objective: The purpose of this study was to examine the effectiveness of adding agility and perturbation techniques to standard exercise therapy compared with the standard exercise program alone for people with knee OA.
Design: This was a single-blinded randomized controlled trial.
Setting: The study was conducted in the outpatient physical therapy clinic of a large, university-based health center.
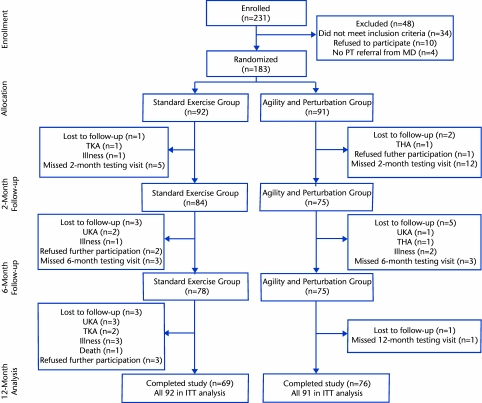
Participants: One hundred eighty-three people with knee OA (122 women, 61 men) participated.
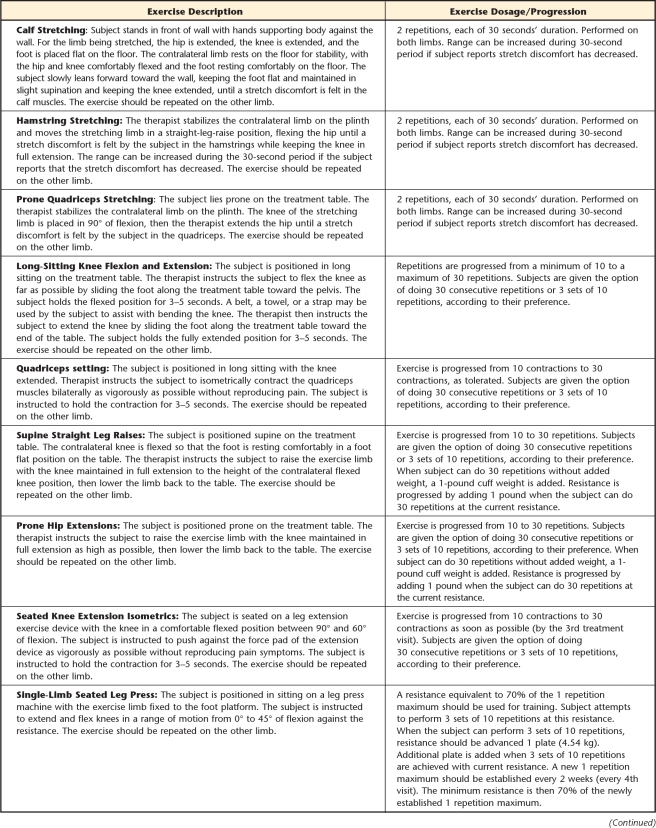
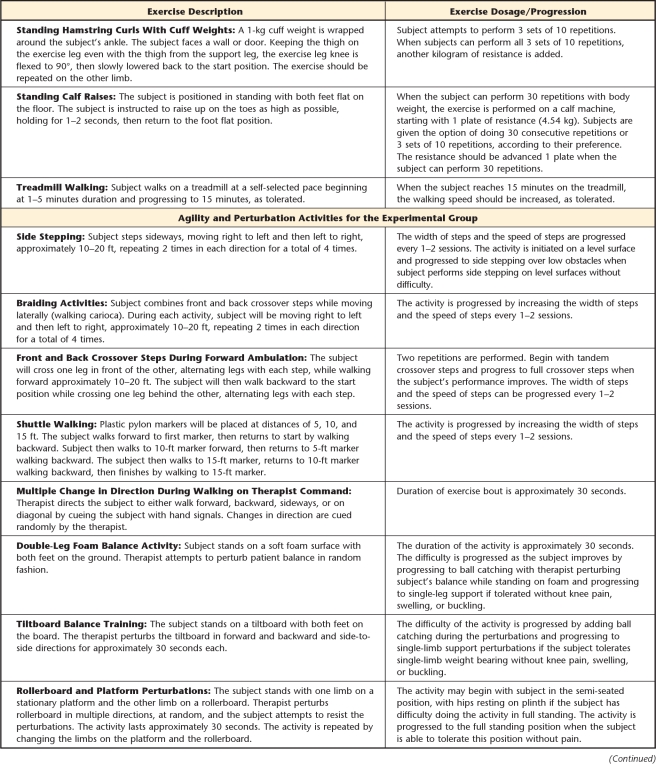
Interventions: Participants were randomly assigned to either a group that received agility and perturbation training with standard exercise therapy or a group that received only the standard exercise program.
Measurements: The outcome measures were self-reported knee pain and function, self-reported knee instability, a performance-based measure of function, and global rating of change.
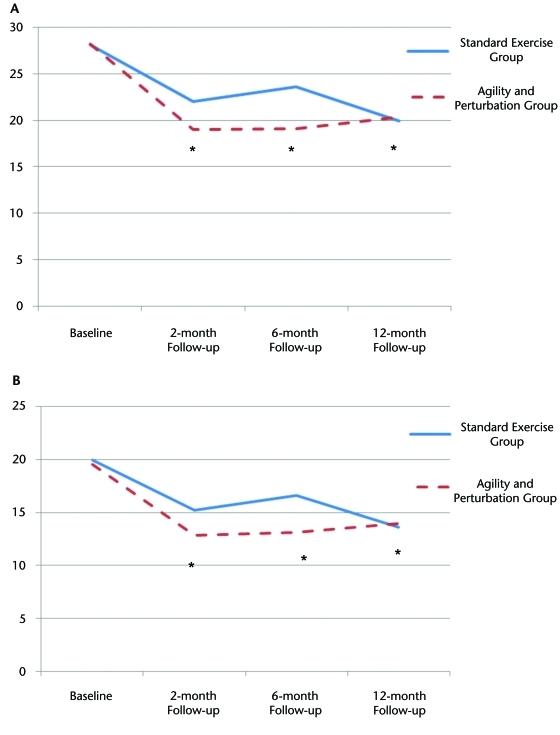
Results: Although both groups exhibited improvement in self-reported function and in the global rating of change at the 2-, 6-, and 12-month follow-up periods, there were no differences between groups on these outcomes. There was no reduction in knee pain or improvement in performance-based function in either group.
Limitations: It is possible that more-intense application of the interventions or application of the interventions to participants with knee OA who were at greater risk for falling may have yielded additive effects of the agility and perturbation training approach.
Conclusions: Both intervention groups exhibited improvement in self-reported function and the global rating of change. Our results, however, did not support an additive effect of agility and perturbation training with standard exercise therapy in our sample of individuals with knee OA. Further study is needed to determine whether there are subgroups of individuals who might achieve an added benefit with this approach.
Trial registration: ClinicalTrials.gov NCT00078624.
Figures
References
-
- American College of Rheumatology Subcommittee on Osteoarthritis Guidelines Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. Arthritis Rheum. 2000;43:1905–1915 - PubMed
-
- Jordan KM, Arden NK, Doherty M, et al. EULAR Recommendations 2003; an evidence-based approach to the management of knee osteoarthritis: report of a task force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis. 2003;62:1145–1155 - PMC - PubMed
-
- Ottawa Panel Evidence-Based Clinical Practice Guidelines for Therapeutic Exercises and Manual Therapy in the Management of Osteoarthritis. Phys Ther. 2005;85:907–971 - PubMed
-
- Zhang W, Moskowitz RW, Nuki G, et al. OARSI recommendations for the management of hip and knee osteoarthritis, part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis Cartilage. 2008;16:137–162 - PubMed
-
- Fransen M, McConnell S, Bell M. Exercise for osteoarthritis of the hip or knee. Cochrane Database Syst Rev. 2003;3:CD004286. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
