

Accurate positioning for head and neck cancer patients using 2D and 3D image guidance
- PMID: 21330971
- PMCID: PMC3065820
- DOI: 10.1120/jacmp.v12i1.3270
Accurate positioning for head and neck cancer patients using 2D and 3D image guidance
Abstract
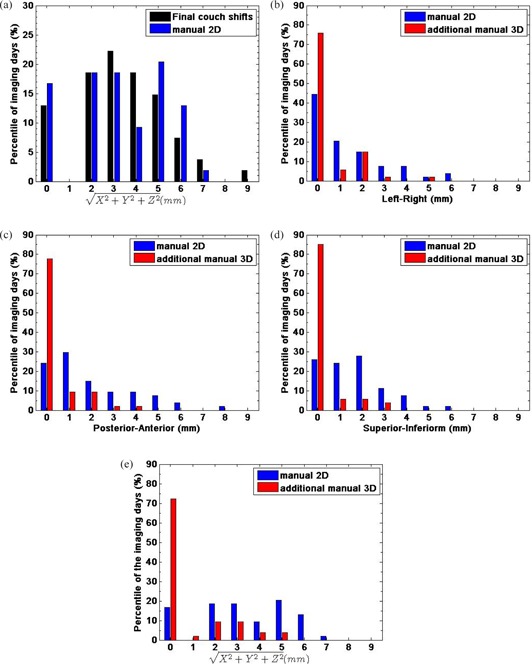
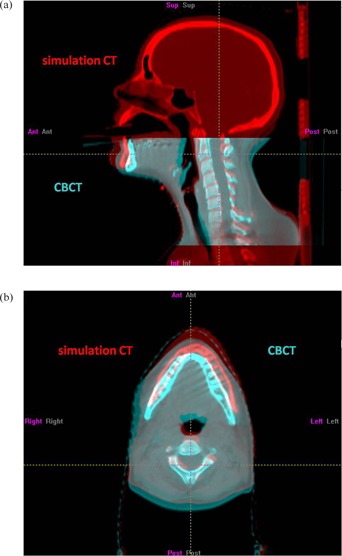
Our goal is to determine an optimized image-guided setup by comparing setup errors determined by two-dimensional (2D) and three-dimensional (3D) image guidance for head and neck cancer (HNC) patients immobilized by customized thermoplastic masks. Nine patients received weekly imaging sessions, for a total of 54, throughout treatment. Patients were first set up by matching lasers to surface marks (initial) and then translationally corrected using manual registration of orthogonal kilovoltage (kV) radiographs with DRRs (2D-2D) on bony anatomy. A kV cone beam CT (kVCBCT) was acquired and manually registered to the simulation CT using only translations (3D-3D) on the same bony anatomy to determine further translational corrections. After treatment, a second set of kVCBCT was acquired to assess intrafractional motion. Averaged over all sessions, 2D-2D registration led to translational corrections from initial setup of 3.5 ± 2.2 (range 0-8) mm. The addition of 3D-3D registration resulted in only small incremental adjustment (0.8 ± 1.5 mm). We retrospectively calculated patient setup rotation errors using an automatic rigid-body algorithm with 6 degrees of freedom (DoF) on regions of interest (ROI) of in-field bony anatomy (mainly the C2 vertebral body). Small rotations were determined for most of the imaging sessions; however, occasionally rotations > 3° were observed. The calculated intrafractional motion with automatic registration was < 3.5 mm for eight patients, and < 2° for all patients. We conclude that daily manual 2D-2D registration on radiographs reduces positioning errors for mask-immobilized HNC patients in most cases, and is easily implemented. 3D-3D registration adds little improvement over 2D-2D registration without correcting rotational errors. We also conclude that thermoplastic masks are effective for patient immobilization.
Figures


References
-
- Hurkmans CW, Remeijer P, Lebesque JV, Mijnheer BJ. Set‐up verification using portal imaging; review of current clinical practice. Radiother Oncol. 2001;58(2):105–20. - PubMed
-
- Gilbeau L, Scalliet P, Grégoire V. Comparison of setup accuracy of three different thermoplastic masks for the treatment of brain and head and neck tumors. Radiother Oncol. 2001;58(2):155–62. - PubMed
-
- Georg D, Bogner J, Dieckmann K, Pötter R. Is mask‐based stereotactic head‐and‐neck fixation as precise as stereotactic head fixation for precision radiotherapy? Int J Radiat Oncol Biol Phys. 2006;66(4, Suppl 1):S61–S66.
-
- Lawson JD, Fox T, Elder E, et al. Early clinical experience with kilovoltage image‐guided radiation therapy for interfraction motion management. Med Dosim. 2008;33(4):268–74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
