

Computed tomography findings of unanticipated prolonged ileocolic intussusception in children
- PMID: 21331206
- PMCID: PMC3037120
- DOI: 10.7812/TPP/08-003
Computed tomography findings of unanticipated prolonged ileocolic intussusception in children
Abstract
Background: Attempted nonsurgical reduction of ileocolic intussusceptions after 48 hours is controversial because of the low probability of reduction and an increased risk of perforation. We sought to retrospectively identify computed tomography (CT) criteria that may help to predict bowel viability and successful enema reduction in children with ileocolic intussusception.
Methods: Unanticipated intussusception was diagnosed using CT in six children with mild, atypical symptoms of four to seven days' duration at a single institution during a one-year period. All patients underwent laparotomy without prior contrast enema. Surgical findings were compared with preoperative CT scan findings to identify any criteria that may predict successful nonsurgical management.
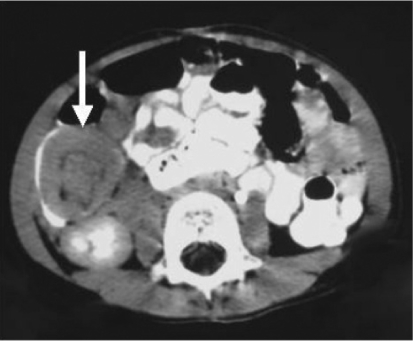
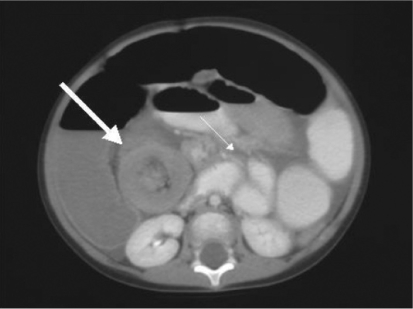
Results: Contrast CT scan findings were diagnostic of ileocolic intussusception. At the time of laparotomy, three children had easily reducible ileocolic intussusception with nonischemic bowel. Two children had irreducible intussusception with ischemic bowel requiring resection, and one child had a difficult reduction of nonischemic but edematous bowel. Preoperative CT scan findings correlated well with intraoperative findings for all patients. Findings of bowel-wall edema of the intussuscipiens and partial small-bowel obstruction shown on CT were associated with intussusception that was nonreducible or difficult to reduce.
Conclusion: Patients with prolonged intussusception diagnosed using CT scan may safely undergo contrast enema reduction if no bowel-wall edema of the intussuscipiens or obstruction is demonstrated.
Figures
Similar articles
-
Radiographic findings predictive of irreducibility and surgical resection in ileocolic intussusception.Pediatr Radiol. 2020 Aug;50(9):1249-1254. doi: 10.1007/s00247-020-04695-0. Epub 2020 Jun 9. Pediatr Radiol. 2020. PMID: 32519054
-
Outcomes in pediatric patients with documented delays between ileocolic intussusception diagnosis and therapeutic enema attempt: evaluation of reduction efficacy and complication rate.Emerg Radiol. 2022 Dec;29(6):953-959. doi: 10.1007/s10140-022-02079-5. Epub 2022 Jul 30. Emerg Radiol. 2022. PMID: 35907145
-
Role of surgery in the era of highly successful air enema reduction of intussusception.Asian J Surg. 2006 Oct;29(4):267-73. doi: 10.1016/S1015-9584(09)60101-9. Asian J Surg. 2006. PMID: 17098661
-
Twenty years' experience for reduction of ileocolic intussusceptions by saline enema under sonography control.J Pediatr Surg. 2016 Jan;51(1):179-82. doi: 10.1016/j.jpedsurg.2015.09.022. Epub 2015 Oct 8. J Pediatr Surg. 2016. PMID: 26592955 Review.
-
Intestinal Intussusception: Etiology, Diagnosis, and Treatment.Clin Colon Rectal Surg. 2017 Feb;30(1):30-39. doi: 10.1055/s-0036-1593429. Clin Colon Rectal Surg. 2017. PMID: 28144210 Free PMC article. Review.
References
-
- Lui KW, Wong HF, Cheung YC, et al. Air enema for diagnosis and reduction of intussusception in children: clinical experience and fluoroscopy time correlation. J Pediatr Surg. 2001 Mar;36(3):479–81. - PubMed
-
- Okuyama H, Nakai H, Okada A. Is barium enema reduction safe and effective in patients with a long duration of intussusception? Pediatr Surg Int. 1999;15(2):105–7. - PubMed
-
- Sandler AD, Ein SH, Connolly B, Daneman A, Filler RM. Unsuccessful air-enema reduction of intussusception: is a second attempt worthwhile? Pediatr Surg Int. 1999;15(3–4):214–6. - PubMed
-
- Ein SH, Mercer S, Humphry A, Macdonald P. Colon perforation during attempted barium enema reduction of intussusception. J Pediatr Surg. 1981 Jun;16(3):313–5. - PubMed
LinkOut - more resources
Full Text Sources
