

Early postoperative MRI overestimates residual tumour after resection of gliomas with no or minimal enhancement
- PMID: 21331595
- PMCID: PMC3101346
- DOI: 10.1007/s00330-011-2081-y
Early postoperative MRI overestimates residual tumour after resection of gliomas with no or minimal enhancement
Abstract
Background: Standards for residual tumour measurement after resection of gliomas with no or minimal enhancement have not yet been established. In this study residual volumes on early and late postoperative T2-/FLAIR-weighted MRI are compared.
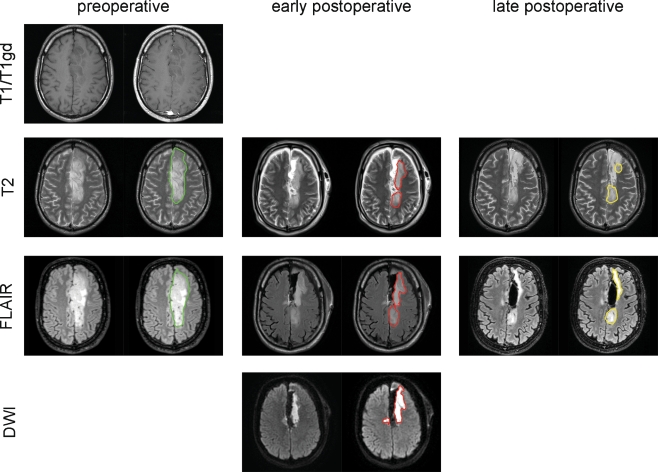
Methods: A retrospective cohort included 58 consecutive glioma patients with no or minimal preoperative gadolinium enhancement. Inclusion criteria were first-time resection between 2007 and 2009 with a T2-/FLAIR-based target volume and availability of preoperative, early (<48 h) and late (1-7 months) postoperative MRI. The volumes of non-enhancing T2/FLAIR tissue and diffusion restriction areas were measured.
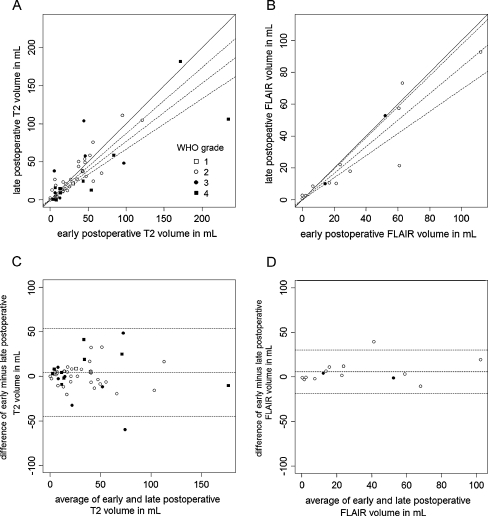
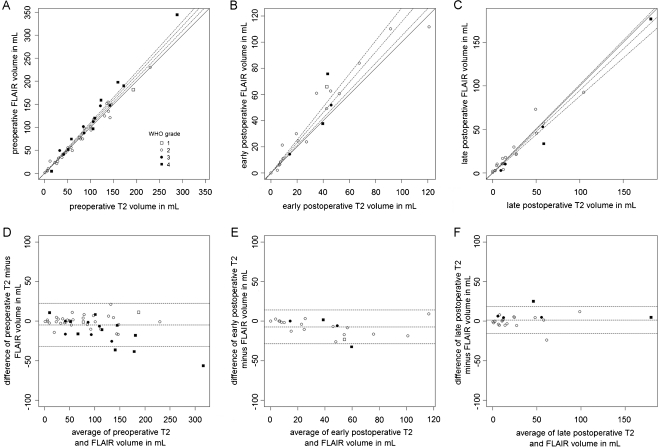
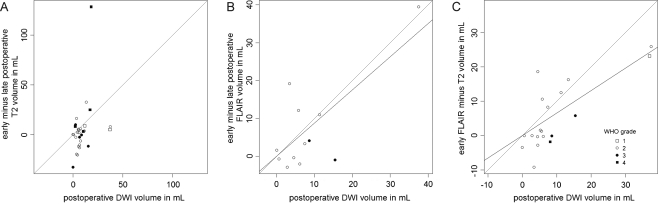
Results: Residual tumour volumes were 22% smaller on late postoperative compared with early postoperative T2-weighted MRI and 49% smaller for FLAIR-weighted imaging. Postoperative restricted diffusion volume correlated with the difference between early and late postoperative FLAIR volumes and with the difference between T2 and FLAIR volumes on early postoperative MRI.
Conclusion: We observed a systematic and substantial overestimation of residual non-enhancing volume on MRI within 48 h of resection compared with months postoperatively, in particular for FLAIR imaging. Resection-induced ischaemia contributes to this overestimation, as may other operative effects. This indicates that early postoperative MRI is less reliable to determine the extent of non-enhancing residual glioma and restricted diffusion volumes are imperative.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
