

Abdominal pain after gastric bypass: suspects and solutions
- PMID: 21333269
- PMCID: PMC3123682
- DOI: 10.1016/j.amjsurg.2010.05.007
Abdominal pain after gastric bypass: suspects and solutions
Abstract
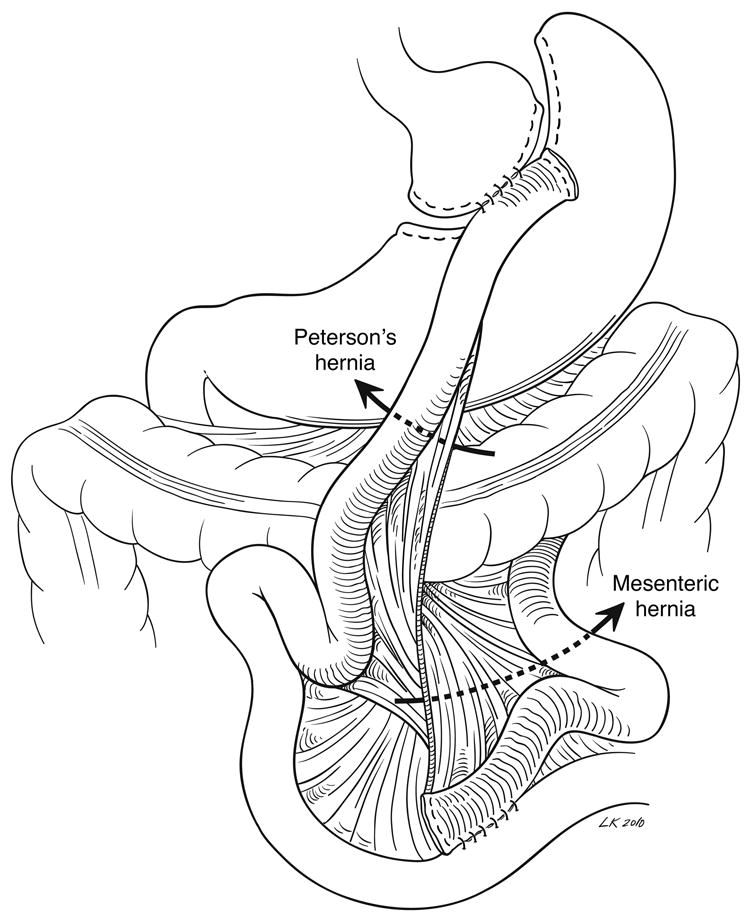
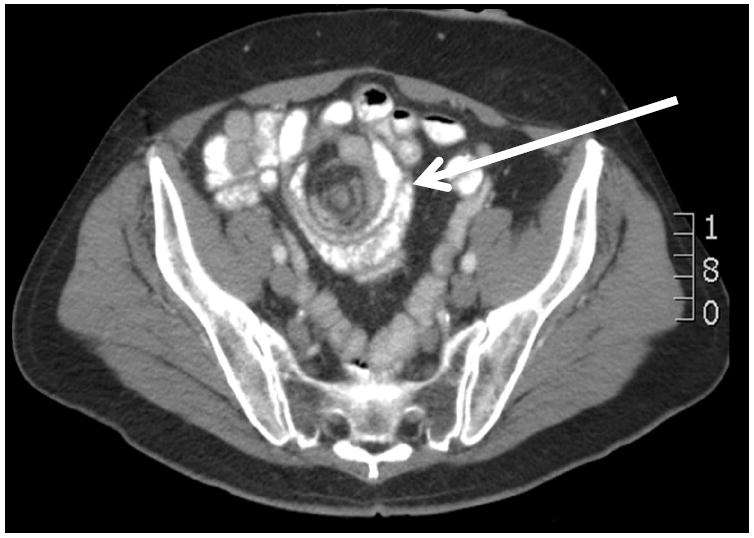
Background: Gastric bypass remains the mainstay of surgical therapy for obesity. Abdominal pain after gastric bypass is common and accounts for up to half of all postoperative complaints and emergency room visits. This article reviews the most important causes of abdominal pain specific to gastric bypass and discusses management considerations.
Methods: The current surgical literature was reviewed using PubMed, with a focus on abdominal pain after gastric bypass and the known pathologies that underlie its pathogenesis.
Results: The etiologies of abdominal pain after gastric bypass are diverse. A thorough understanding of their pathogenesis impacts favorably on clinical outcomes.
Conclusions: The differential diagnosis for abdominal pain after gastric bypass is large and includes benign and life-threatening entities. Its diverse causes require a broad evaluation that should be directed by history and clinical presentation. In the absence of a clear diagnosis, the threshold for surgical exploration in patients with abdominal pain after gastric bypass should be low.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
References
-
- Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric surgical procedures. JAMA. 2005;294:1909–1917. - PubMed
-
- Cho M, Kaidar-Person O, Szomstein S, Rosenthal RJ. Emergency room visits after laparoscopic Roux-en-Y gastric bypass for morbid obesity. Surg Obes Relat Dis. 2008;4(2):104–9. - PubMed
-
- Saunders J, Ballantyne GH, Belsley S, Stephens DJ, Trivedi A, Ewing DR, Iannace VA, Capella RF, Wasileweski A, Moran S, Schmidt HJ. One-year readmission rates at a high volume bariatric surgery center: laparoscopic adjustable gastric banding, laparoscopic gastric bypass, and vertical banded gastroplasty-Roux-en-Y gastric bypass. Obes Surg. 2008;18(10):1233–40. - PubMed
-
- Kellogg TA, Swan T, Leslie DA, Buchwald H, Ikramuddin S. Patterns of readmission and reoperation within 90 days after Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2009;5(4):416–23. - PubMed
-
- Foster A, Richards WO, McDowell J, Laws HL. Clements RH. Gastrointestinal symptoms are more intense in morbidly obese patients. Surg Endosc. 2003;17(11):1766–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
