

Long-term oxandrolone treatment increases muscle protein net deposition via improving amino acid utilization in pediatric patients 6 months after burn injury
- PMID: 21333314
- PMCID: PMC3079061
- DOI: 10.1016/j.surg.2010.12.006
Long-term oxandrolone treatment increases muscle protein net deposition via improving amino acid utilization in pediatric patients 6 months after burn injury
Abstract
Background: We recently showed that mechanisms of protein turnover in skeletal muscle are unresponsive to amino acid (AA) infusion in severely burned pediatric patients at 6 months postinjury. In the current study, we evaluated whether oxandrolone treatment affects mechanisms of protein turnover in skeletal muscle and whole-body protein breakdown in pediatric burn patients 6 months postinjury.
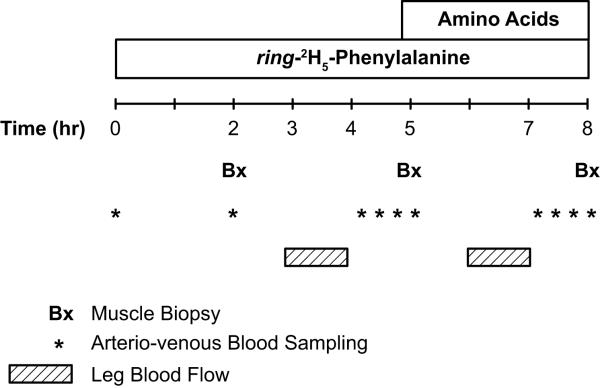
Methods: At the time of admission, patients were randomized to control or oxandrolone treatments. The treatment regimens were continued until 6 months postinjury, at which time patients (n = 26) underwent study with a stable isotope tracer infusion to measure muscle and whole-body protein turnover.
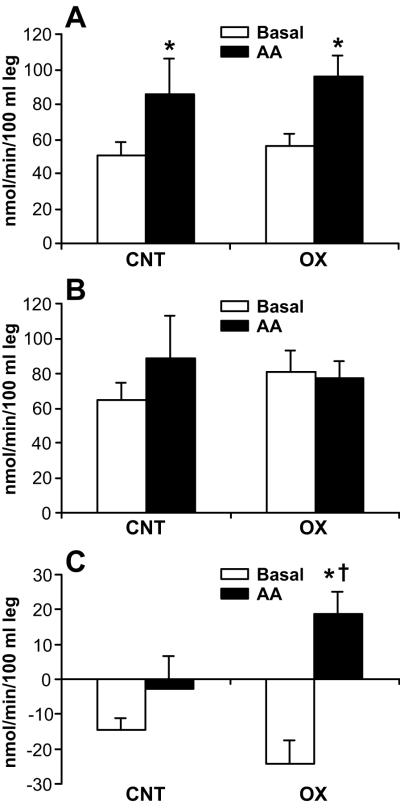
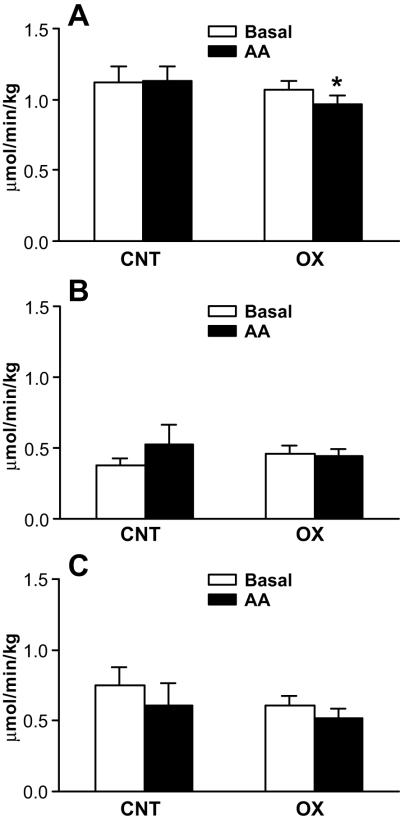
Results: Protein kinetics in leg muscle were expressed in nmol/min per 100 mL leg volume (mean ± SE). During AA infusion, rates of protein synthesis in leg muscle were increased (P < .05) in both groups (basal vs AA: control, 51 ± 8 vs 86 ± 21; oxandrolone, 56 ± 7 vs 96 ± 12). In the control group, there was also a simultaneous increase in breakdown (basal vs AA: 65 ± 10 vs 89 ± 25), which resulted in no change in the net balance of leg muscle protein (basal vs AA: -15 ± 4 vs -2 ± 10). In the oxandrolone group, protein breakdown did not change (basal vs AA: 80 ± 12 vs 77 ± 9), leading to increased net balance (basal vs AA: -24 ± 7 vs 19 ± 7; P < .05). Protein breakdown at the whole-body level was not different between the groups.
Conclusion: Long-term oxandrolone treatment increased net deposition of leg muscle protein during AA infusion by attenuating protein breakdown, but did not affect whole-body protein breakdown.
Copyright © 2011 Mosby, Inc. All rights reserved.
Figures
References
-
- Hart DW, Wolf SE, Mlcak R, Chinkes DL, Ramzy PI, Obeng MK, et al. Persistence of muscle catabolism after severe burn. Surgery. 2000;128:312–9. - PubMed
-
- Fox M, Minot AS, Liddle GW. Oxandrolone: a potent anabolic steroid of novel chemical configuration. J Clin Endocrinol metab. 1962;22:921–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
