

3D visualization of subdural electrode shift as measured at craniotomy reopening
- PMID: 21334178
- PMCID: PMC4329774
- DOI: 10.1016/j.eplepsyres.2011.01.011
3D visualization of subdural electrode shift as measured at craniotomy reopening
Abstract
Purpose: Subdural electrodes are implanted for recording intracranial EEG (iEEG) in cases of medically refractory epilepsy as a means to locate cortical regions of seizure onset amenable to surgical resection. Without the aid of imaging-derived 3D electrode models for surgical planning, surgeons have relied on electrodes remaining stationary from the time between placement and follow-up resection. This study quantifies electrode shift with respect to the cortical surface occurring between electrode placement and subsequent reopening.
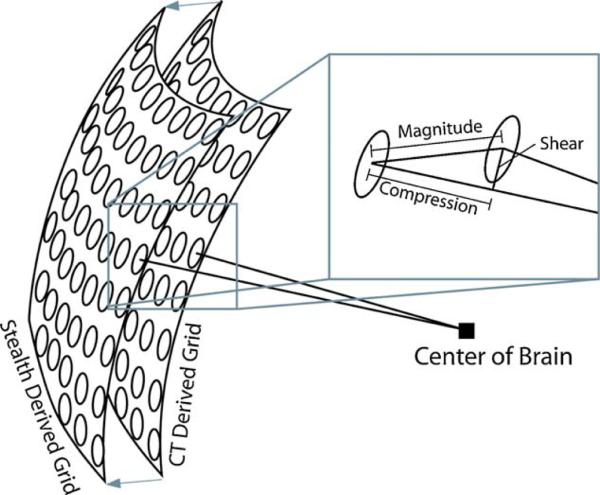
Methods: CT and structural MRI data were gathered following electrode placement on 10 patients undergoing surgical epilepsy treatment. MRI data were used to create patient specific post-grid 3D reconstructions of cortex, while CT data were co-registered to the MRI and thresholded to reveal electrodes only. At the time of resective surgery, the craniotomy was reopened and electrode positions were determined using intraoperative navigational equipment. Changes in position were then calculated between CT coordinates and intraoperative electrode coordinates.
Results: Five out of ten patients showed statistically significant overall magnitude differences in electrode positions (mean: 7.2mm), while 4 exhibited significant decompression based shift (mean: 4.7mm), and 3 showed significant shear displacement along the surface of the brain (mean: 7.1mm).
Discussion: Shift in electrode position with respect to the cortical surface has never been precisely measured. We show that in 50% of our cases statistically significant shift occurred. These observations demonstrate the potential utility of complimenting electrode position measures at the reopening of the craniotomy with 3D electrode and brain surface models derived from post-implantation CT and MR imaging for better definition of surgical boundaries.
Copyright © 2011 Elsevier B.V. All rights reserved.
Figures



Similar articles
-
Quantification of Subdural Electrode Shift Between Initial Implantation, Postimplantation Computed Tomography, and Subsequent Resection Surgery.Oper Neurosurg. 2019 Jan 1;16(1):9-19. doi: 10.1093/ons/opy050. Oper Neurosurg. 2019. PMID: 29617890 Free PMC article.
-
Investigation of subdural electrode displacement in invasive epilepsy surgery workup using neuronavigation and intraoperative MRI.Neurol Res. 2018 Oct;40(10):811-821. doi: 10.1080/01616412.2018.1484588. Epub 2018 Jun 19. Neurol Res. 2018. PMID: 29916770
-
Intraoperative computed tomography for intracranial electrode implantation surgery in medically refractory epilepsy.J Neurosurg. 2015 Mar;122(3):526-31. doi: 10.3171/2014.9.JNS13919. Epub 2014 Oct 31. J Neurosurg. 2015. PMID: 25361483
-
Depths and grids in brain tumors: implantation strategies, techniques, and complications.Epilepsia. 2013 Dec;54 Suppl 9:66-71. doi: 10.1111/epi.12447. Epilepsia. 2013. PMID: 24328876 Review.
-
Neuronavigation applied to epilepsy monitoring with subdural electrodes.Neurosurg Focus. 2008 Sep;25(3):E21. doi: 10.3171/FOC/2008/25/9/E21. Neurosurg Focus. 2008. PMID: 18759623 Review.
Cited by
-
Advances in human intracranial electroencephalography research, guidelines and good practices.Neuroimage. 2022 Oct 15;260:119438. doi: 10.1016/j.neuroimage.2022.119438. Epub 2022 Jul 2. Neuroimage. 2022. PMID: 35792291 Free PMC article. Review.
-
Surface based electrode localization and standardized regions of interest for intracranial EEG.Hum Brain Mapp. 2018 Feb;39(2):709-721. doi: 10.1002/hbm.23876. Epub 2017 Nov 2. Hum Brain Mapp. 2018. PMID: 29094783 Free PMC article.
-
Electrode localization for planning surgical resection of the epileptogenic zone in pediatric epilepsy.Int J Comput Assist Radiol Surg. 2014 Jan;9(1):91-105. doi: 10.1007/s11548-013-0915-6. Epub 2013 Jun 23. Int J Comput Assist Radiol Surg. 2014. PMID: 23793723 Free PMC article.
-
Intracranial EEG surface renderings: new insights into normal and abnormal brain function.Neuroscientist. 2013 Jun;19(3):238-47. doi: 10.1177/1073858412447876. Epub 2012 May 31. Neuroscientist. 2013. PMID: 22653695 Free PMC article.
-
Modeling intracranial electrodes. A simulation platform for the evaluation of localization algorithms.Front Neuroinform. 2022 Oct 6;16:788685. doi: 10.3389/fninf.2022.788685. eCollection 2022. Front Neuroinform. 2022. PMID: 36277477 Free PMC article.
References
-
- Behrens E, Zentner J, van Roost D, Hufnagel A, Elger CE, Schramm J. Subdural and depth electrodes in the presurgical evaluation of epilepsy. Acta Neurochir. (Wien) 1994;128:84–87. - PubMed
-
- Bootsveld K, Traber F, Kaiser WA, Layer G, Elger CE, Hufnagel A, Gieseke J, Reiser M. [Intracranial ECoG electrodes Location determination using three-dimensional reconstruction of MR data of the brain as a component of the presurgical diagnosis of epilepsy]. Radiologe. 1993;33:185–188. - PubMed
-
- Dale AM, Fischl B, Sereno MI. Cortical surface-based analysis I. Segmentation and surface reconstruction. Neuroimage. 1999;9:179–194. - PubMed
-
- Engel J, Jr., Henry TR, Risinger MW, Mazziotta JC, Sutherling WW, Levesque MF, Phelps ME. Presurgical evaluation for partial epilepsy: relative contributions of chronic depth-electrode recordings versus FDG-PET and scalp-sphenoidal ictal EEG. Neurology. 1990;40:1670–1677. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
