

Inhibition of ventilatory motor output increases expiratory retro palatal compliance during sleep
- PMID: 21334465
- PMCID: PMC3143713
- DOI: 10.1016/j.resp.2011.02.007
Inhibition of ventilatory motor output increases expiratory retro palatal compliance during sleep
Abstract
We hypothesized that inhibition of ventilatory motor output leads to increased pharyngeal compliance during NREM sleep, independent of lung volume.
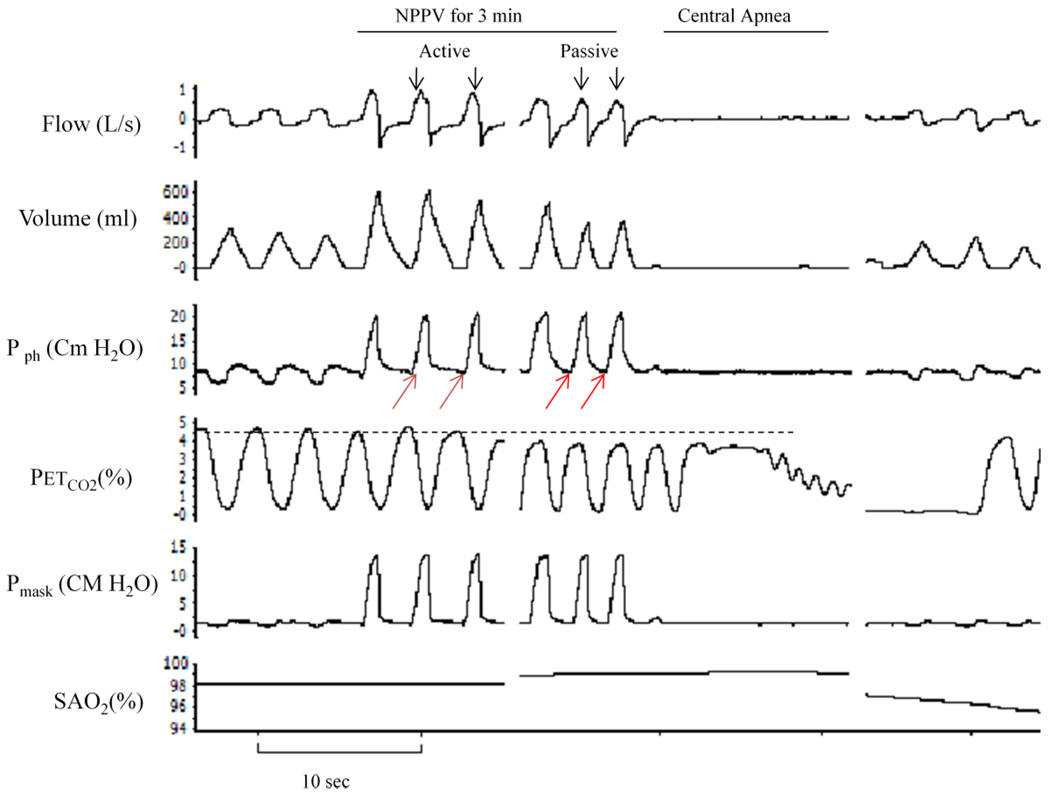
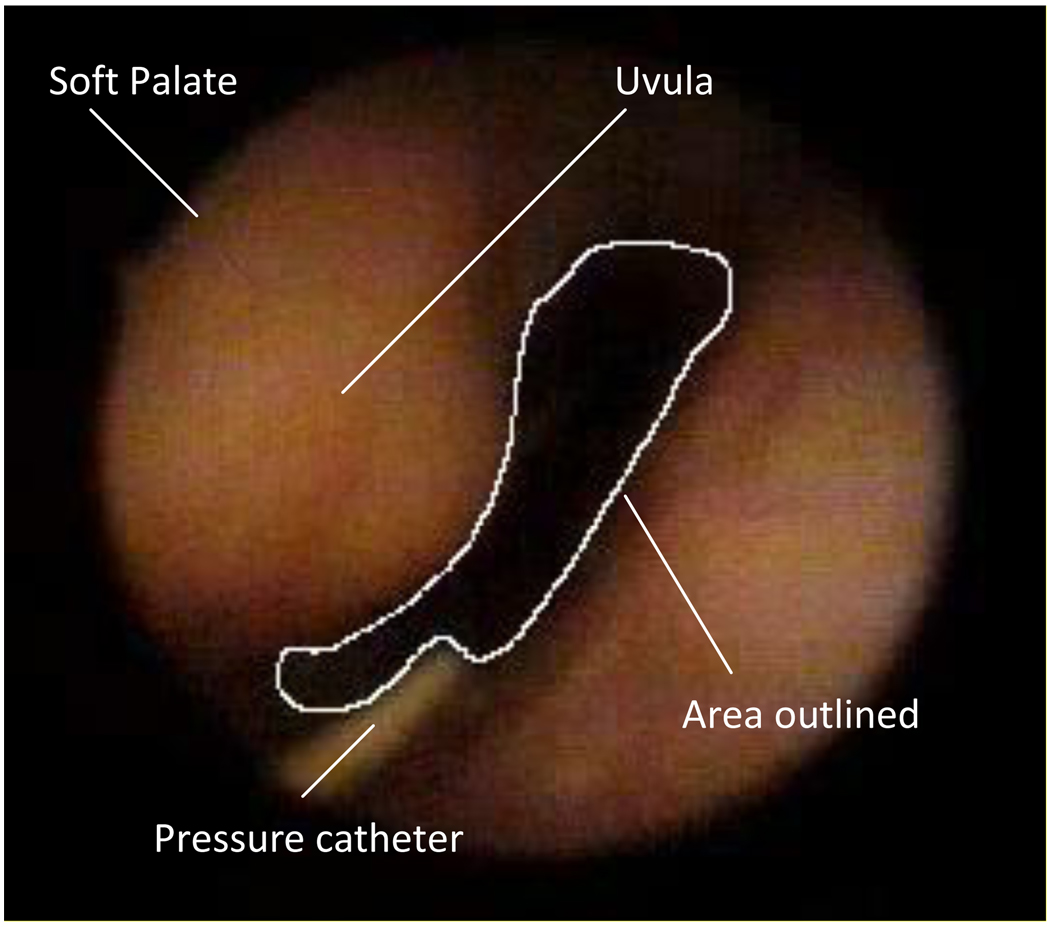
Methods: Eighteen subjects were studied using noninvasive positive pressure ventilation (NPPV) to inhibit ventilatory motor output during stable NREM sleep. Nasopharyngoscopy was used to measure the retro palatal cross-sectional area/pressure relationship (CSA/Pph) in 8 subjects. The effect of NPPV on neck circumference (NC) and end-expiratory lung volumes (EELV) was studied in 10 additional subjects using strain gauge plethysmography and respitrace, respectively.
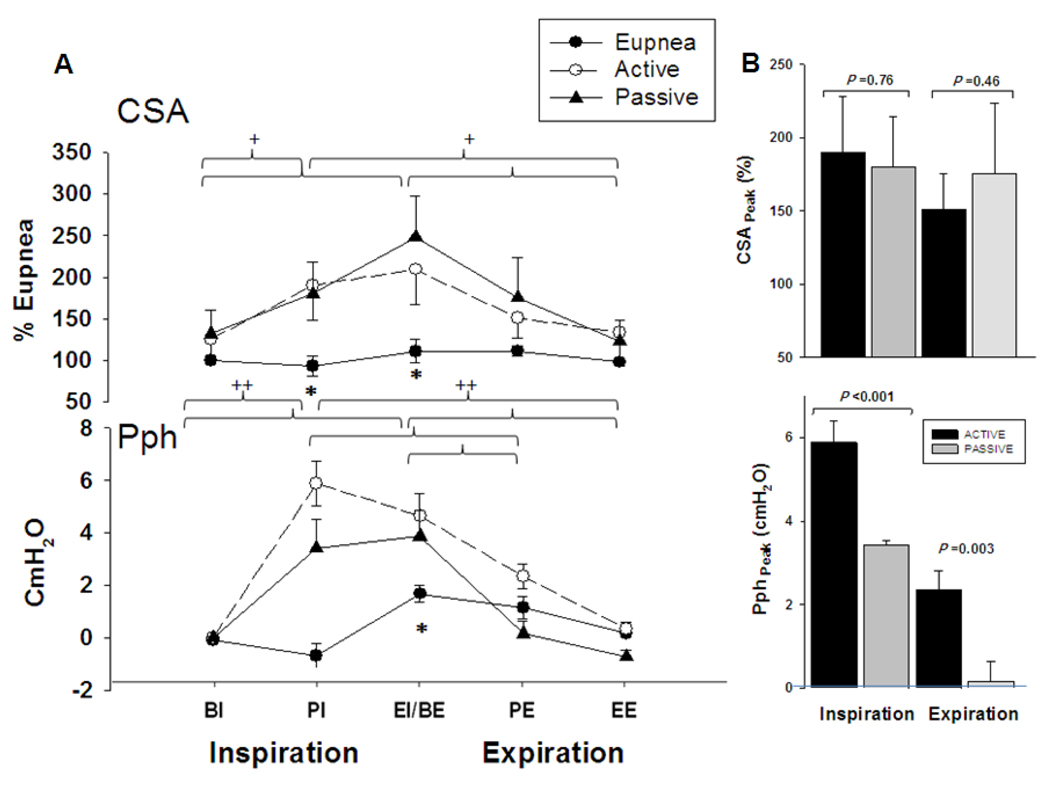
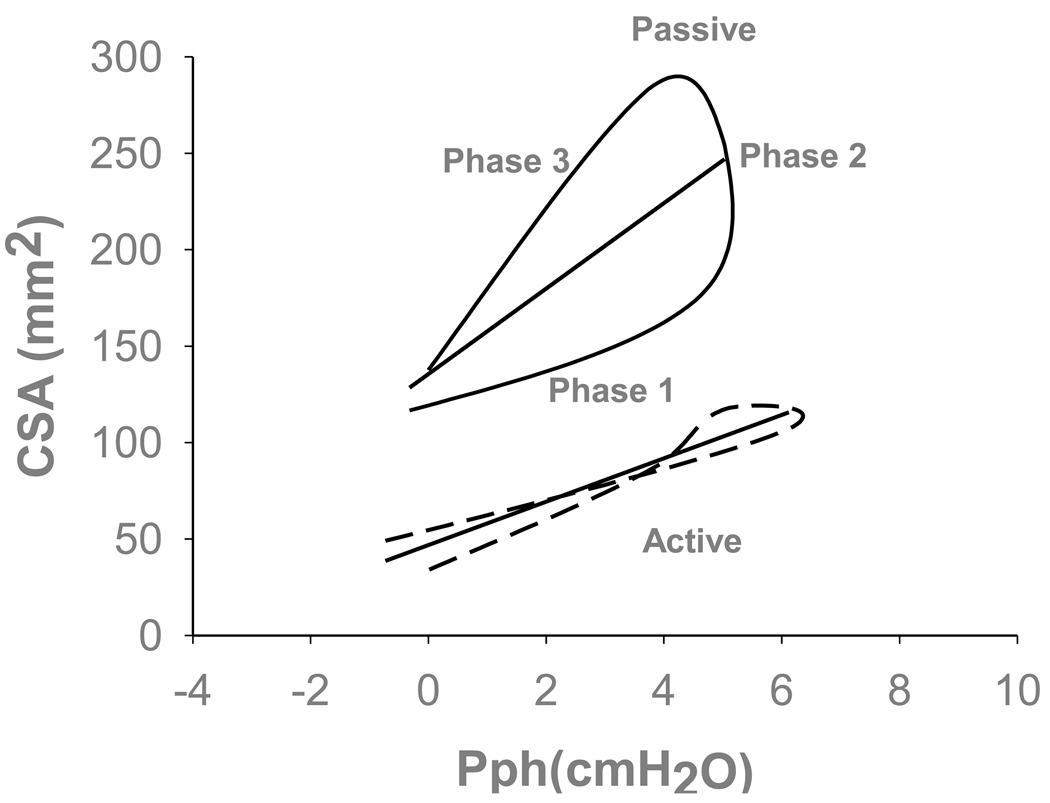
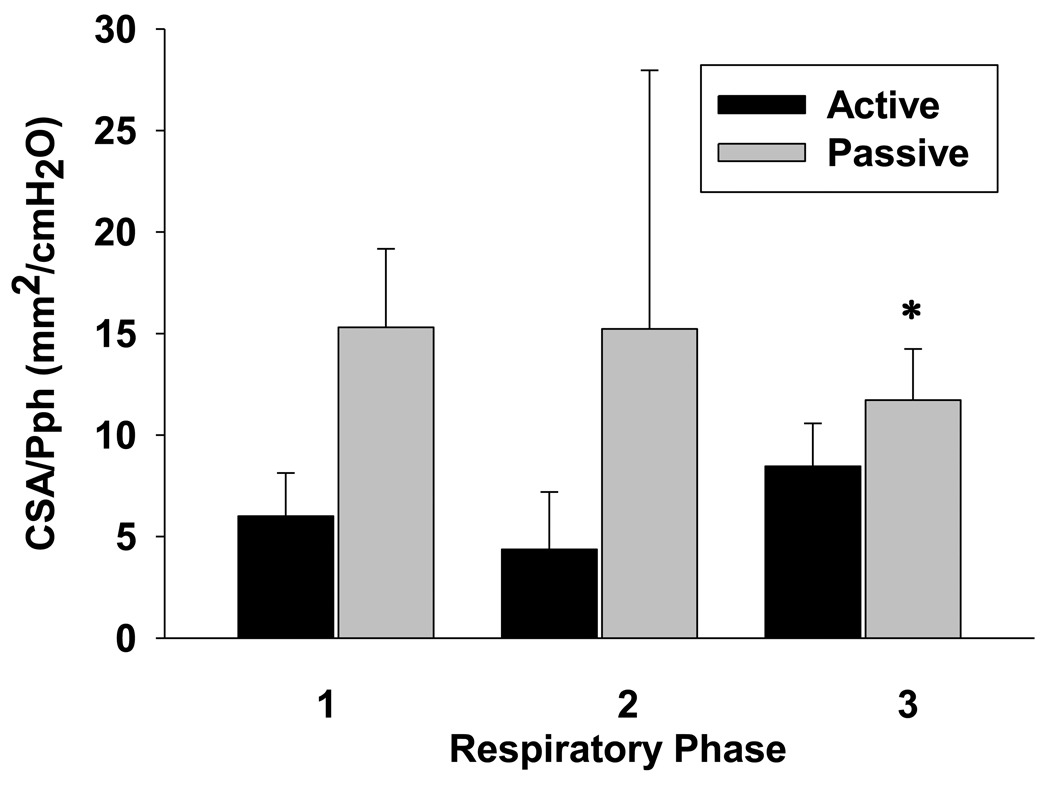
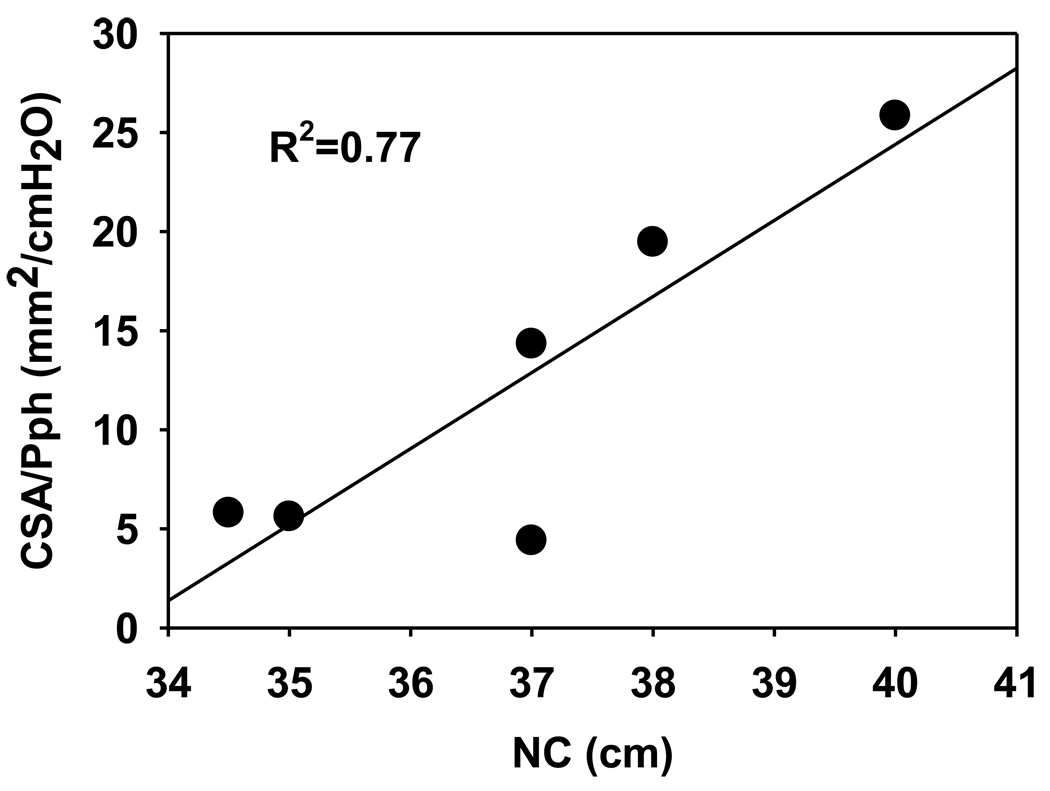
Results: (1) The CSA/Pph was increased during expiration under passive compared to active breathing (11.7 ± 7.1 vs. 8.5 ± 5.6mm(2)/cmH(2)O, respectively; p < 0.05) but not during inspiration. (2) NC correlated with the CSA/Pph during passive expiration (R(2) = 0.77, p < 0.05). (3) NC and EELV did not change between active and passive breaths (p = NS).
Conclusions: (1) Inhibiting the ventilatory motor output increases the pharyngeal compliance. (2) Increased passive expiratory pharyngeal compliance was not associated with changes in NC or EELV.
Published by Elsevier B.V.
Figures

References
-
- Alex CG, Aronson RM, Onal E, et al. Effects of continuous positive airway pressure on upper airway and respiratory muscle activity. J.Appl.Physiol. 1987;62(5):2026–2030. - PubMed
-
- Badr MS, Toiber F, Skatrud JB, et al. Pharyngeal narrowing/occlusion during central sleep apnea. J.Appl.Physiol. 1995;78(5):1806–1815. - PubMed
-
- Badr MS. Effect of ventilatory drive on upper airway patency in humans during NREM sleep. Respir.Physiol. 1996;103(1):1–10. - PubMed
-
- Borowiecki B, Pollak CP, Weitzman ED, et al. Fibro-optic study of pharyngeal airway during sleep in patients with hypersomnia obstructive sleep-apnea syndrome. Laryngoscope. 1978;88(8 Pt 1):1310–1313. - PubMed
-
- Condos R, Norman RG, Krishnasamy I, et al. Flow limitation as a noninvasive assessment of residual upper-airway resistance during continuous positive airway pressure therapy of obstructive sleep apnea. Am.J.Respir.Crit Care Med. 1994;150(2):475–480. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
