

Comparison between pedicle subtraction osteotomy and anterior corpectomy and plating for correcting post-traumatic kyphosis: a multicenter study
- PMID: 21336510
- PMCID: PMC3175905
- DOI: 10.1007/s00586-011-1720-y
Comparison between pedicle subtraction osteotomy and anterior corpectomy and plating for correcting post-traumatic kyphosis: a multicenter study
Abstract
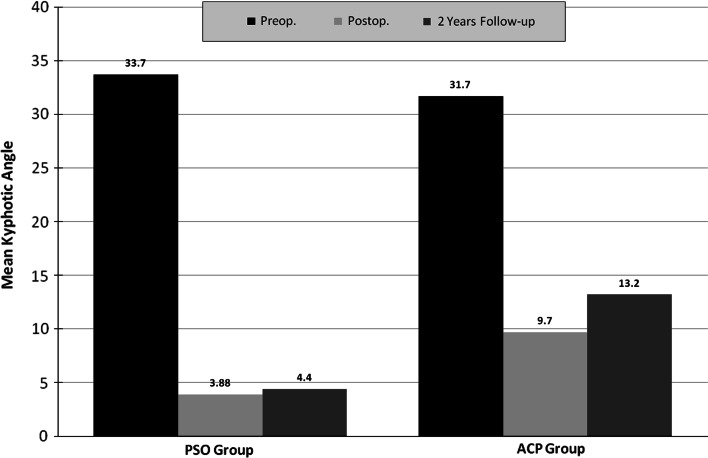
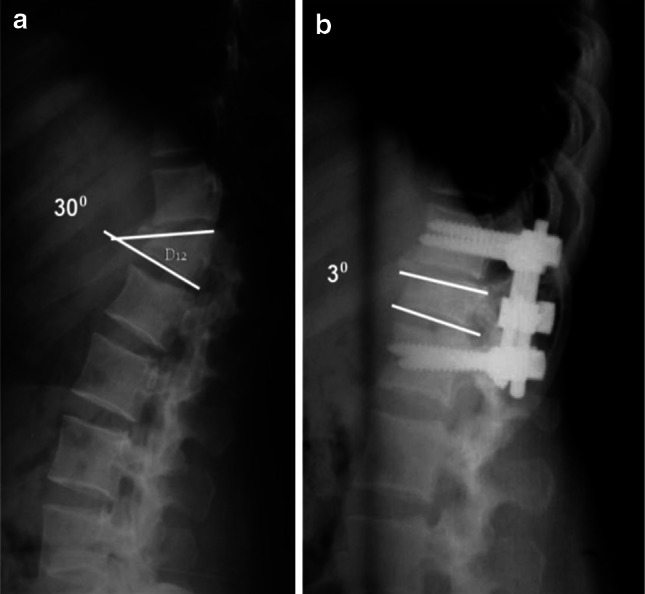
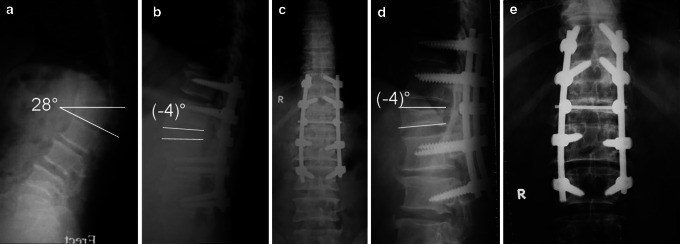
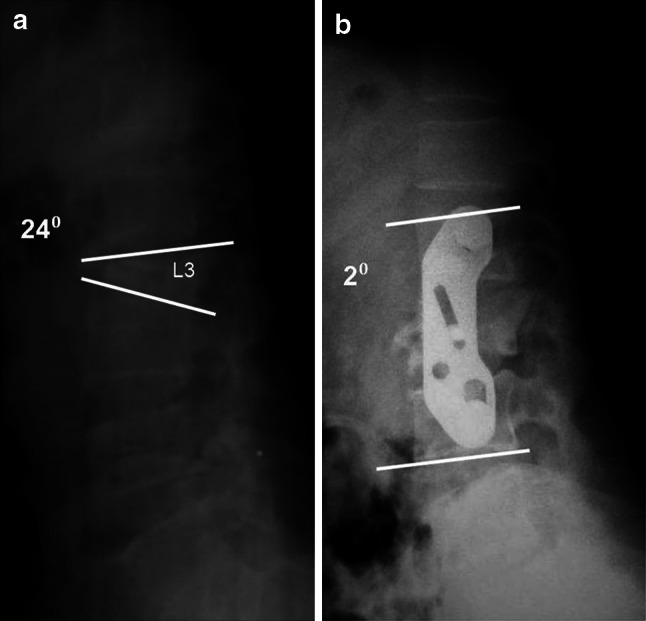
Kyphosis is a common sequel of inadequately managed thoracolumbar fractures. This study compares between pedicle subtraction osteotomy (PSO) and anterior corpectomy and plating (ACP) for correcting post-traumatic kyphosis. Forty-three patients with symptomatic post-traumatic kyphosis of the thoracolumbar spine were treated with PSO and prospectively followed for a minimum of 2 years. Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI) were used to assess clinical improvement and radiographs were obtained at 2, 6, 12 and 24 months. The recorded clinical and radiological outcomes were compared to a control group of 37 patients, who were treated earlier by the same authors with ACP. The mean correction of the kyphotic angle was 29.8° for the PSO group and 22° for the ACP group (P = 0.001). PSO group showed significantly better improvement in the VAS score and the ODI. At final follow-up, patients reported very good satisfaction (93% in PSO vs. 81% in ACP) and good function (90% in PSO vs. 73% in ACP). Complications in the PSO group included pulling out of screws and recurrence of deformity requiring revision and longer fixation (1 patient), and transient lower limb paraesthesia (2 patients). Recorded complications in the ACP group included an aortic injury (1 patient) that was successfully repaired, pseudarthrosis (1 patient), persistent graft donor site morbidity (3 patients), and incisional hernia (1 patient). PSO and ACP are demanding procedures. PSO seems to be equally safe but more effective than ACP for correcting post-traumatic kyphosis.
Figures

References
-
- Malcolm BW, Bradford DS, Winter RB, Chou SN. Post-traumatic kyphosis: a review of forty-eight surgically treated patients. J Bone Joint Surg Am. 1981;63:891–899. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
