

Hyperglycemia is a strong prognostic factor of lethality in methanol poisoning
- PMID: 21336799
- PMCID: PMC3550199
- DOI: 10.1007/s13181-011-0142-x
Hyperglycemia is a strong prognostic factor of lethality in methanol poisoning
Abstract
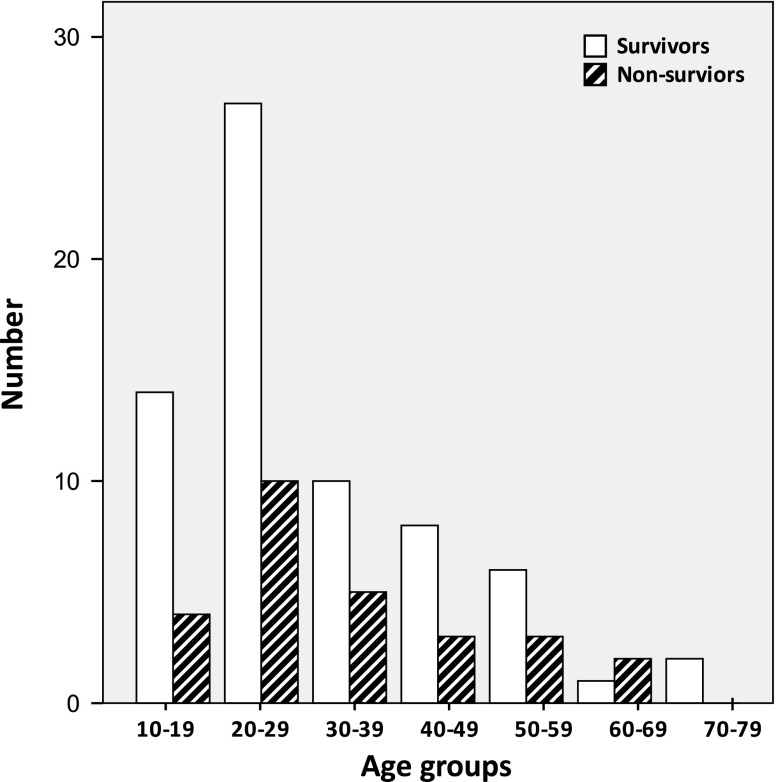
Methanol poisoning is seen in the form of isolated episodes, or intentional ingestion and epidemics. Despite its efficient treatment, methanol poisoning has high morbidity and mortality rates. So far, several studies have been performed to identify the prognostic factors in methanol poisoning. Recently, during the treatment of patients with methanol poisoning, we observed that patients' blood glucose levels were high on presentation to the hospital, particularly in those who expired. Through a literature search, we found that no studies have been performed on blood glucose levels or hyperglycemia in methanol poisoning. Therefore, the present retrospective study was done as a preliminary investigation to understand whether there was a meaningful relationship between methanol poisoning and blood glucose level on presentation, and also if hyperglycemia could be considered as a prognostic factor for mortality. In this retrospective study, a review of the hospital charts was performed for all patients who were treated for methanol poisoning from March 2003 to March 2010 in two hospitals in Tehran, Iran. Those with definitive diagnosis of methanol poisoning, no history of diabetes mellitus, and normal or low body mass index (<25) were included. Patients' demographic information, clinical manifestations, time elapsed between ingestion and presentation, blood glucose level on presentation (before treatment), results of arterial blood gas analysis, and the clinical outcome were recorded. Statistical analysis was done using SPSS software (version 17, Chicago, Illinois, USA) and application of Mann-Whitney U test, Pearson's chi-square test, Pearson correlation coefficient (r), receiver operating characteristic (ROC) curve, and logistic regression. P values less than 0.05 were considered as the statistically significant levels. Ninety-five patients with methanol poisoning met the inclusion criteria and were included in the study. Of these, 91 (96%) were male and 4 (4%) were female. Mean age was 31.61 ± 14.3 years (range, 13 to 75). Among the 95 patients, 68 survived (72%) and 27 expired (28%). Median blood glucose level was 144 mg/dL (range, 75 to 500). There was no significant statistical correlation between blood glucose level and time of treatment, age, pCO(2), or serum bicarbonate concentration, but blood glucose level had a statistically significant correlation with pH (r = -0.242, P = 0.02) and base deficit (r = 0.230, P = 0.03). The mean blood glucose level was 140 ± 55 and 219 ± 99 mg/dL in the survivor and non-survivor patients, respectively (P < 001). Considering the cutoff level of 140 mg/dL for blood glucose and using logistic regression analysis, and adjusting according to the admission data with significant statistical difference in the two study groups, the odds ratio for hyperglycemia as a risk factor for death was 6.5 (95% confidence interval = 1.59-26.4). Our study showed that blood glucose levels were high in methanol poisoning and even higher in those who died in comparison with the survivors. Therefore, hyperglycemia might be a new prognostic factor in methanol poisoning, but further studies are needed to determine whether controlling hyperglycemia has therapeutic consequences.
Figures
References
-
- Barceloux DG, Bond GR, Krenzelok EP, Cooper H, Vale JA, American Academy of Clinical Toxicology Ad Hoc Committee on the Treatment Guidelines for Methanol Poisoning American Academy of Clinical Toxicology practice guidelines on the treatment of methanol poisoning. J Toxicol Clin Toxicol. 2002;40(4):415–446. doi: 10.1081/CLT-120006745. - DOI - PubMed
-
- Jacobsen D, McMartin KE. Methanol and ethylene glycol poisonings. Mechanism of toxicity, clinical course, diagnosis and treatment. Med Toxicol. 1986;1(5):309–334. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
