

Predictive factors for functional improvement after intravitreal bevacizumab therapy for macular edema due to branch retinal vein occlusion
- PMID: 21337042
- PMCID: PMC3042100
- DOI: 10.1007/s00417-010-1470-2
Predictive factors for functional improvement after intravitreal bevacizumab therapy for macular edema due to branch retinal vein occlusion
Abstract
Background: To identify predictive factors for improvement of visual acuity and central retinal thickness by intravitreal bevacizumab for the treatment of macular edema (ME) due to branch retinal vein occlusion (BRVO).
Methods: Two hundred and five eyes from 204 patients with ME secondary to BRVO were retrospectively included at six sites. All eyes received intravitreal bevacizumab therapy (1.25 mg/0.05 ml). The mean follow-up was 36.8 ± 12.7 weeks (range, 18 to 54 weeks). Measurement of ETDRS best-corrected visual acuity (BCVA, in all eyes) and optical coherence tomography (OCT, in 87% of eyes) were performed at baseline and at follow-up examinations every 12 weeks. Using fluorescein angiography, the perfusion status of the macula at baseline could be assessed in 84% of the eyes. The main outcome measures were changes in BCVA and central retinal thickness (CRT). For analysis of predictive factors, the results at 24 weeks were used.
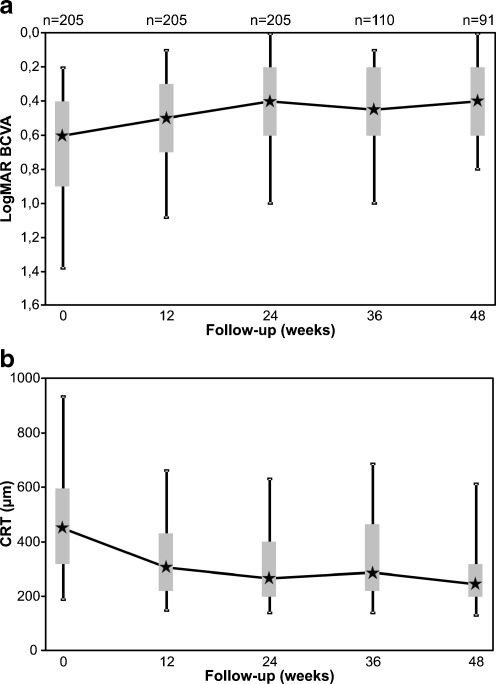
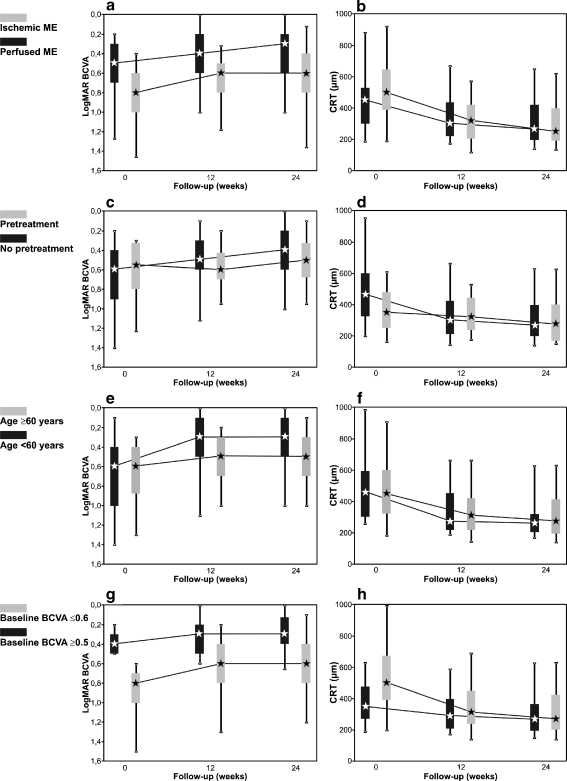
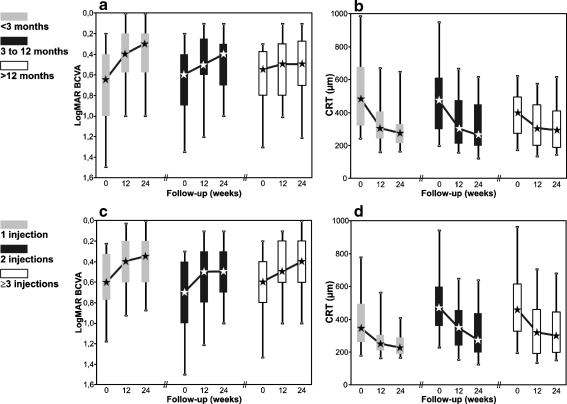
Results: The median BCVA was 0.6 LogMAR at baseline and improved to 0.4 LogMAR at 24 and 48 weeks. This visual improvement was associated by a significant reduction in CRT, decreasing from a baseline of 454 μm to 267 μm and 248 μm after 24 and 48 weeks respectively. Eyes with ME and intact (perfused) or interrupted (ischemic) foveal capillary ring showed a 2-line increase of median BCVA [45 eyes (22%) and 128 eyes (62%) respectively]. However, the final median BCVA was significantly worse in eyes with ischemic ME (0.6 versus 0.3 logMAR in perfused ME). Other factors for visual improvement were absence of previous treatments of the ME, age younger than 60 years and low baseline BCVA (≥0.6 logMAR) (2, 3, and 2 median BCVA lines increase respectively). Furthermore, eyes with duration of the ME of less than 12 months responded with a 3-line increase of the median BCVA. Final CRT only showed minor differences between the subgroups. During the entire follow-up, retreatments were performed in 85% of the eyes, with a median number of injections of three (mean 3.2; range, 1 to 10) and a median time-interval between injections of 11.6 weeks (mean 14.6 weeks).
Conclusions: Intravitreal injection of bevacizumab resulted in a significant improvement of BCVA and reduction of ME in BRVO. Baseline BCVA, patient's age, and duration of BRVO were found to be of prognostic relevance for visual improvement. A less favorable outcome of the bevacizumab therapy in eyes with longstanding BRVO would advocate initiation of treatment within 12 months after onset.
Figures
References
-
- The Branch Vein Occlusion Study Group Argon laser photocoagulation for macular edema in branch vein occlusion. Am J Ophthalmol. 1984;98:271–282. - PubMed
-
- The SCORE Study Research Group A randomized trial comparing the efficacy and safety of intravitreal triamcinolone with standard care to treat vision loss associated with macular edema secondary to branch retinal vein occlusion: the standard care vs corticosteroid for retinal vein occlusion (SCORE) study report 6. Arch Ophthalmol. 2009;127:1115–1128. doi: 10.1001/archophthalmol.2009.233. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
