

Phase II trial of tipifarnib and radiation in children with newly diagnosed diffuse intrinsic pontine gliomas
- PMID: 21339191
- PMCID: PMC3064607
- DOI: 10.1093/neuonc/noq202
Phase II trial of tipifarnib and radiation in children with newly diagnosed diffuse intrinsic pontine gliomas
Abstract
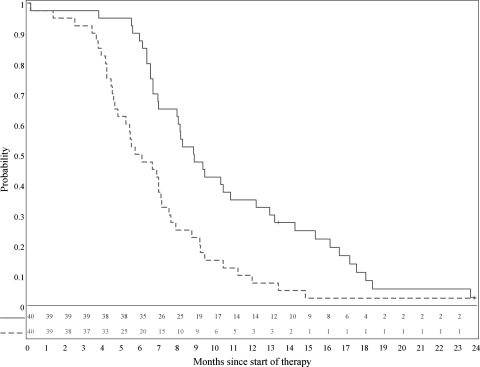
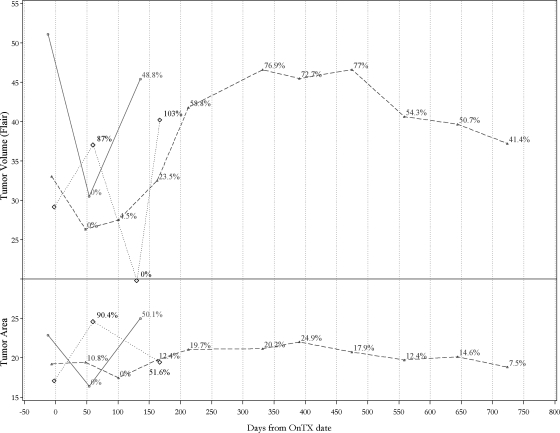
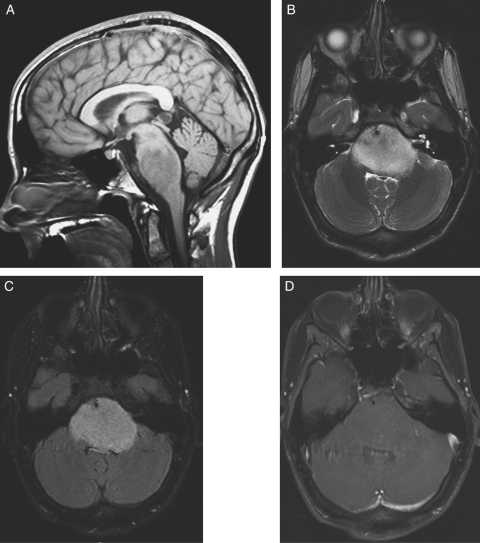
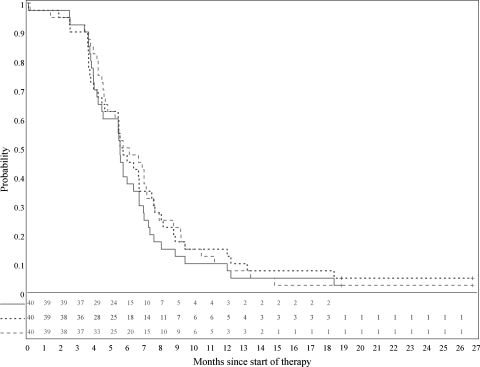
We performed a phase II study to assess the efficacy and toxicity of tipifarnib, a farnesyltransferase inhibitor, administered with radiation therapy (RT) in children with newly diagnosed diffuse intrinsic pontine gliomas. Children 3-21 years old with pontine gliomas (BSGs) were treated with concurrent tipifarnib and RT, followed by adjuvant tipifarnib. Tipifarnib was taken orally twice daily (125 mg/m(2)/dose) during RT; after RT, it was taken at 200 mg/m(2) twice daily for 21 days, in 28-day cycles. Initial and follow-up neuroimaging was centrally reviewed. Forty eligible patients (median age, 5.5 years; range, 3.3-16.5 years) had a median progression-free survival of 6.8 months (range, 0.2-18.6 months) and median overall survival of 8.3 months (range, 0.2-18.6 months). Kaplan-Meier estimates (± standard error) of 1-year progression-free and overall survival were 12.9% ±4.9% and 34.3% ±7.4%, respectively. A single patient remained on tipifarnib without progression at the completion of the study, two years after initiation of treatment. Seven patients were without disease progression for at least six months, three of whom remained controlled for more than a year. The most frequent toxicity was grade 3 lymphopenia. We documented a single instance of "pseudoprogression" by neuroimaging review. We found no discordance among 3 approaches to defining disease progression: as interpreted by treating institutions (based on clinical status and/or imaging) and by central review (using bi-dimensional tumor "area" versus volumetric measurements). For children with diffuse BSGs, tipifarnib administered with irradiation offered no clinical advantage over historical controls. Biopsies and molecular analyses of pediatric BSGs are vital for identification of new agents and for rational use of targeted agents.
Figures
References
-
- Freeman CR, Farmer JP. Pediatric brain stem gliomas: a review. Int J Radiat Oncol Biol Phys. 1998;40:265–271. - PubMed
-
- Fangusaro J. Pediatric high-grade gliomas and diffuse intrinsic pontine gliomas. J Child Neurol. 2009;24(11):1409–1417. - PubMed
-
- Prendergast GC. Farnesyltransferase inhibitors: antineoplastic mechanism and clinical prospects. Curr Opin Cell Biol. 2000;12:166–173. - PubMed
-
- Prendergast GC, Oliff A. Farnesyltransferase inhibitors: antineoplastic properties, mechanisms of action, and clinical prospects. Semin Cancer Biol. 2000;10:443–452. - PubMed
-
- Gilbertson RJ, Hill DA, Hernan R, et al. ERBB1 is amplified and overexpressed in high-grade diffusely infiltrative pediatric brain stem glioma. Clin Cancer Res. 2003;9:3620–3624. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
