

Controversies in the adjuvant therapy of high-grade gliomas
- PMID: 21339260
- PMCID: PMC3228107
- DOI: 10.1634/theoncologist.2010-0335
Controversies in the adjuvant therapy of high-grade gliomas
Abstract
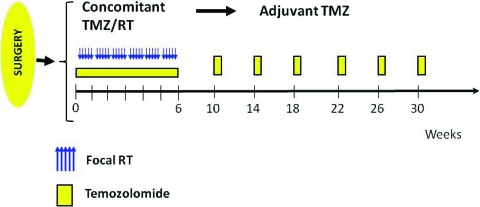
The 2-year survival rate of patients with glioblastoma accrued to research studies increased from 10% to nearly 40% from 2000 to 2010. These improvements began with the demonstration of a survival benefit when daily temozolomide was administered with 6 weeks of standard radiation and for 6 months thereafter. This treatment regimen is often associated with significant lymphopenia, thrombocytopenia, and progressive blood-brain barrier dysfunction that can result in clinical and radiologic deterioration without true tumor progression ("pseudoprogression"). With new evidence that combining this cytotoxic agent with radiation improves survival in this malignancy, many investigators have modified the regimen to further improve patient outcomes. These largely uncontrolled studies highlight controversies regarding the optimal therapy of this disease. This review focuses on the following selected controversies: (a) What is the appropriate temozolomide dose, schedule, and duration in the postradiation period? (b) How should other U.S. Food and Drug Administration-approved therapies (such as carmustine wafers and bevacizumab) be incorporated into this treatment regimen? (c) Should the results in glioblastoma be extrapolated to patients aged >70 and to patients with lower grade gliomas? and (d) How should novel therapeutic approaches be added to radiation and temozolomide in clinical trials for patients with newly diagnosed glioblastoma?
Conflict of interest statement
The content of this article has been reviewed by independent peer reviewers to ensure that it is balanced, objective, and free from commercial bias. No financial relationships relevant to the content of this article have been disclosed by the independent peer reviewers.
Figures
References
-
- Stewart LA. Chemotherapy in adult high-grade glioma: A systematic review and meta-analysis of individual patient data from 12 randomised trials. Lancet. 2002;359:1011–1018. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–996. - PubMed
-
- Stupp R, Hegi ME, Mason WP, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–466. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
