

Endogenous circadian rhythm in vasovagal response to head-up tilt
- PMID: 21339480
- PMCID: PMC3089897
- DOI: 10.1161/CIRCULATIONAHA.110.943019
Endogenous circadian rhythm in vasovagal response to head-up tilt
Abstract
Background: The incidence of syncope exhibits a daily pattern with more occurrences in the morning, possibly as a result of influences from the endogenous circadian system and/or the daily pattern of behavioral/emotional stimuli. This study tested the hypothesis that the circadian system modulates cardiovascular responses to postural stress, leading to increased susceptibility to syncope at specific times of day.
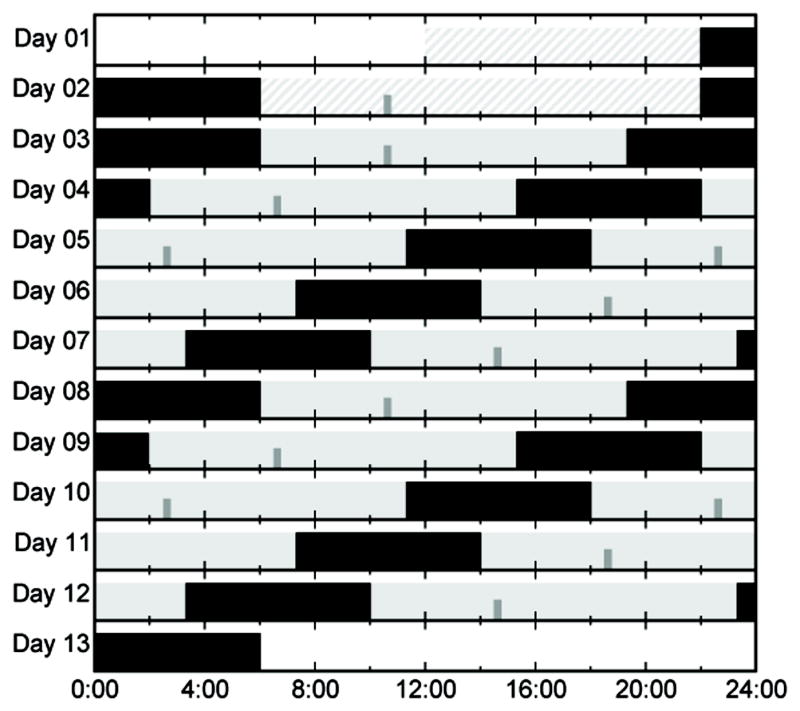
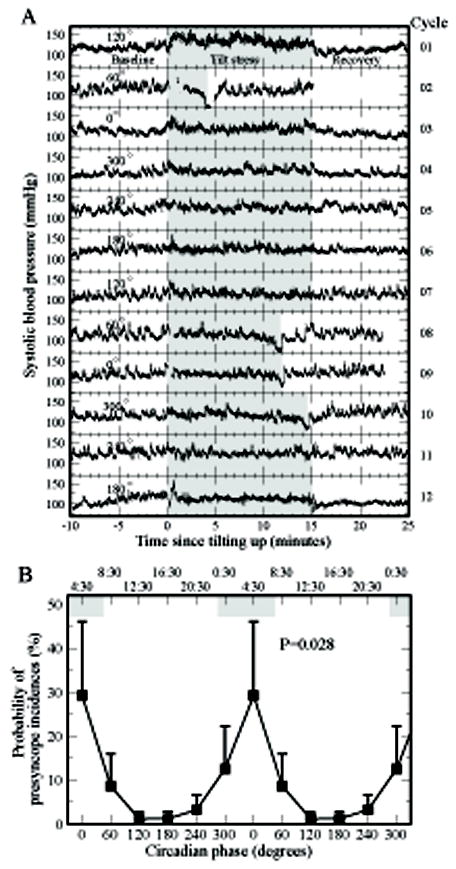
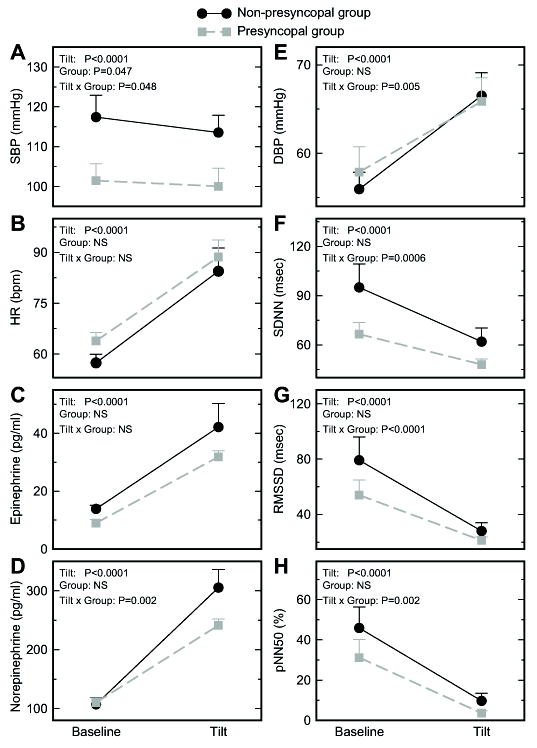
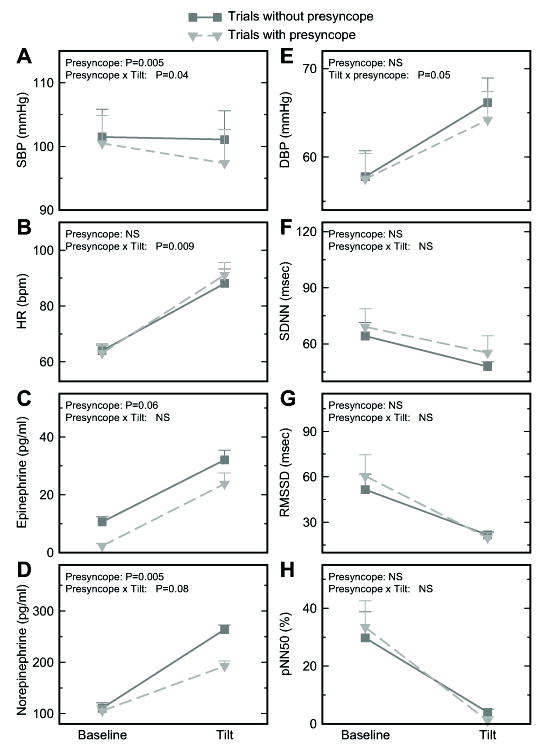
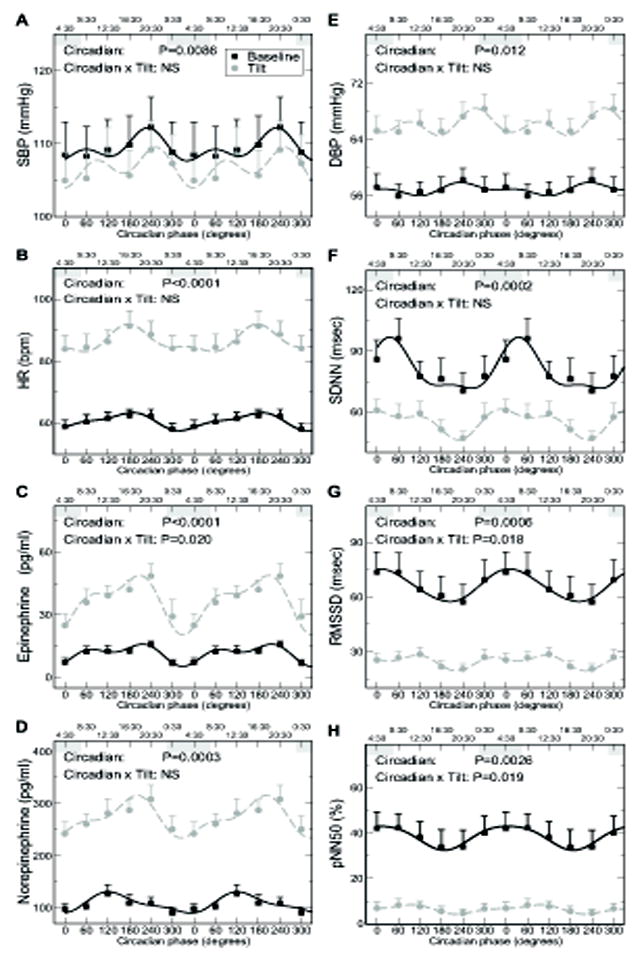
Methods and results: Twelve subjects underwent a 13-day in-laboratory protocol in which subjects' sleep-wake cycles were adjusted to 20 hours for 12 cycles. A 15-minute tilt-table test (60° head-up) was performed ≈4.5 hours after scheduled awakening in each cycle so that 12 tests in each subject were distributed evenly across the circadian cycle. Of 144 tests, signs/symptoms of presyncope were observed in 21 tests in 6 subjects. These presyncope events displayed a clear circadian rhythm (P=0.028) with almost all cases (17/21) occurring in the half of the circadian cycle corresponding to the biological night (10:30 pm to 10:30 am). Significant circadian rhythms were also observed in hemodynamic and autonomic function markers (blood pressure, heart rate, epinephrine, norepinephrine, and indices of cardiac vagal tone) that may underlie the circadian rhythm of presyncope susceptibility.
Conclusions: The circadian system affects cardiovascular responses to postural stress, resulting in greater susceptibility to presyncope during the night. This finding suggests that night-shift workers and people with disrupted sleep at night may have greater risk of syncope as a result of their exposure to postural stress during the biological night.
Figures
Comment in
-
Letter by Ainslie et al regarding article, "Endogenous circadian rhythm in vasovagal response to head-up tilt".Circulation. 2011 Sep 27;124(13):e358; author reply e359. doi: 10.1161/CIRCULATIONAHA.111.032227. Circulation. 2011. PMID: 21947939 No abstract available.
References
-
- The European Society of Cardiology Guidelines for the diagnosis and management of syncope reviewed by Angel Moya, MD, FESC, Chair of the Guideline Taskforce with J. Taylor, MPhil. Eur Heart J. 2009;30:2539–2540. - PubMed
-
- Olde Nordkamp LR, van Dijk N, Ganzeboom KS, Reitsma JB, Luitse JS, Dekker LR, Shen WK, Wieling W. Syncope prevalence in the ED compared to general practice and population: a strong selection process. Am J Emerg Med. 2009;27:271–279. - PubMed
-
- Curtis AB, Epstein AE. Syncope while driving: how safe is safe? Circulation. 2009;120:921–923. - PubMed
-
- Wieling W, Smit AA, de Jong-de Vos van Steenwijk CC, van Lieshout JJ, Karemaker JM. Pathophysiological mechanisms underlying vasovagal syncope in young subjects. Pacing Clin Electrophysiol. 1997;20:2034–2038. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
