

A systematic review and meta-analysis of the efficacy and safety of intermittent preventive treatment of malaria in children (IPTc)
- PMID: 21340029
- PMCID: PMC3038871
- DOI: 10.1371/journal.pone.0016976
A systematic review and meta-analysis of the efficacy and safety of intermittent preventive treatment of malaria in children (IPTc)
Abstract
Background: Intermittent preventive treatment of malaria in children less than five years of age (IPTc) has been investigated as a measure to control the burden of malaria in the Sahel and sub-Sahelian areas of Africa where malaria transmission is markedly seasonal.
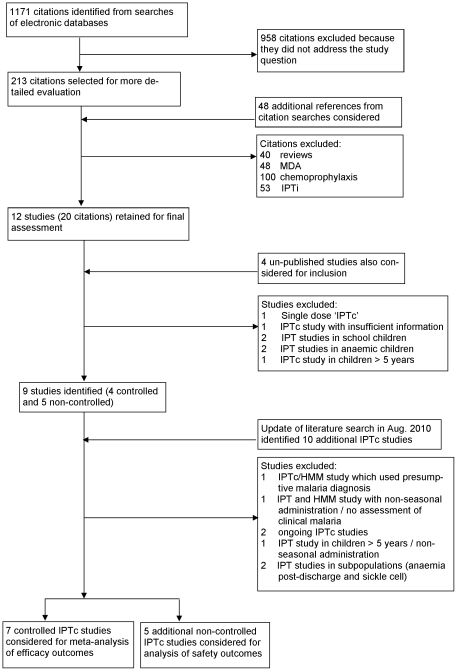
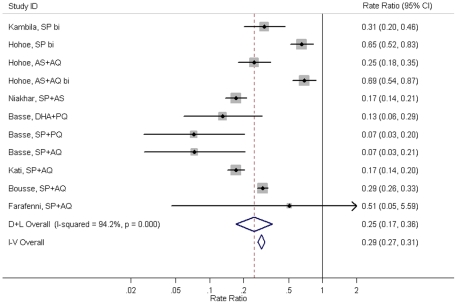
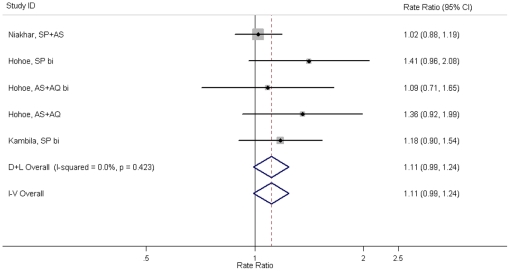
Methods and findings: IPTc studies were identified using a systematic literature search. Meta-analysis was used to assess the protective efficacy of IPTc against clinical episodes of falciparum malaria. The impact of IPTc on all-cause mortality, hospital admissions, severe malaria and the prevalence of parasitaemia and anaemia was investigated. Three aspects of safety were also assessed: adverse reactions to study drugs, development of drug resistance and loss of immunity to malaria. Twelve IPTc studies were identified: seven controlled and five non-controlled trials. Controlled studies demonstrated protective efficacies against clinical malaria of between 31% and 93% and meta-analysis gave an overall protective efficacy of monthly administered IPTc of 82% (95%CI 75%-87%) during the malaria transmission season. Pooling results from twelve studies demonstrated a protective effect of IPTc against all-cause mortality of 57% (95%CI 24%-76%) during the malaria transmission season. No serious adverse events attributable to the drugs used for IPTc were observed in any of the studies. Data from three studies that followed children during the malaria transmission season in the year following IPTc administration showed evidence of a slight increase in the incidence of clinical malaria compared to children who had not received IPTc.
Conclusions: IPTc is a safe method of malaria control that has the potential to avert a significant proportion of clinical malaria episodes in areas with markedly seasonal malaria transmission and also appears to have a substantial protective effect against all-cause mortality. These findings indicate that IPTc is a potentially valuable tool that can contribute to the control of malaria in areas with markedly seasonal transmission.
Conflict of interest statement
Figures
References
-
- Greenwood B. Intermittent preventive treatment - a new approach to the prevention of malaria in children in areas with seasonal malaria transmission. Trop Med Int Health. 2006;11:983–991. - PubMed
-
- World Health Organisation. WHO Policy recommendation on Intermittent Preventive Treatment during infancy with sulphadoxine-pyrimethamine (SP-IPTi) for Plasmodium falciparum malaria control in Africa. 2010.
-
- Aponte JJ, Schellenberg D, Egan A, Breckenridge A, Carneiro I, et al. Efficacy and safety of intermittent preventive treatment with sulfadoxine-pyrimethamine for malaria in African infants: a pooled analysis of six randomised, placebo-controlled trials. The Lancet. 2009;374:1533–1542. - PubMed
-
- Etard JF, Le Hesran JY, Diallo A, Diallo JP, Ndiaye JL, et al. Childhood mortality and probable causes of death using verbal autopsy in Niakhar, Senegal, 1989–2000. Int J Epidemiol. 2004;33:1286–1292. - PubMed
-
- Jaffar S, Leach A, Greenwood AM, Jepson A, Muller O, et al. Changes in the pattern of infant and childhood mortality in upper river division, The Gambia, from 1989 to 1993. Trop Med Int Health. 1997;2:28–37. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
