

Exogenous nitric oxide prevents cardiovascular collapse during hemorrhagic shock
- PMID: 21342744
- PMCID: PMC3081950
- DOI: 10.1016/j.resuscitation.2010.12.025
Exogenous nitric oxide prevents cardiovascular collapse during hemorrhagic shock
Abstract
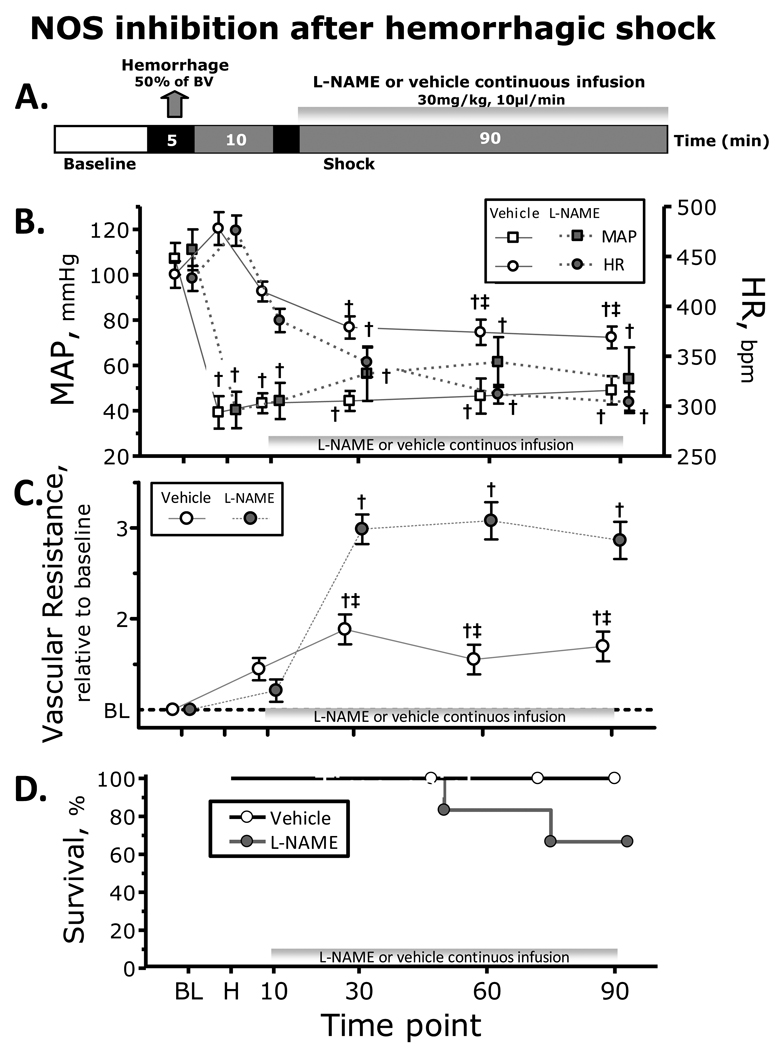
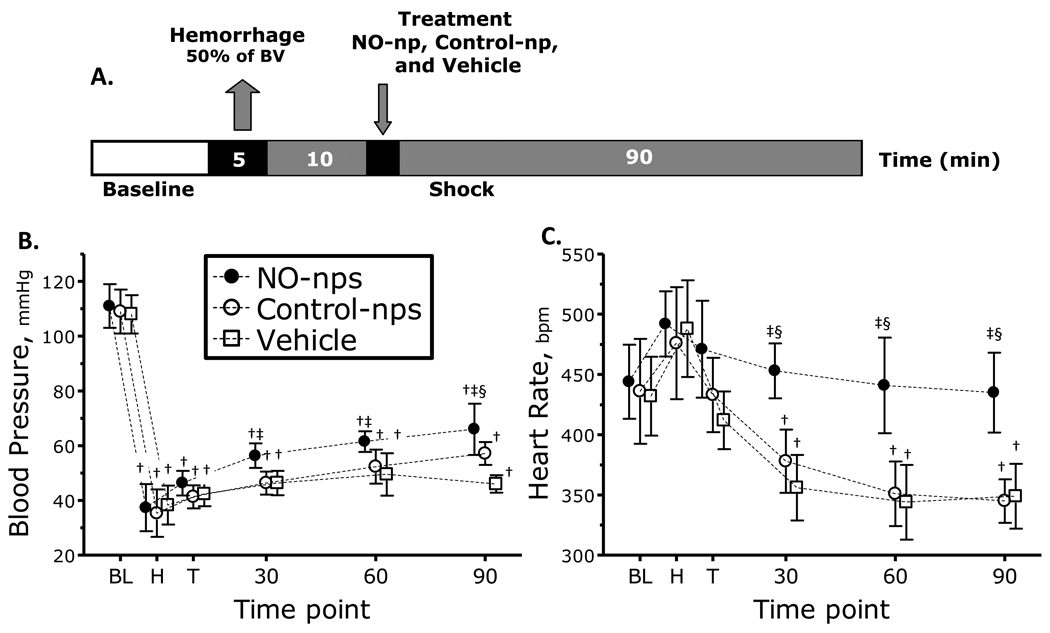
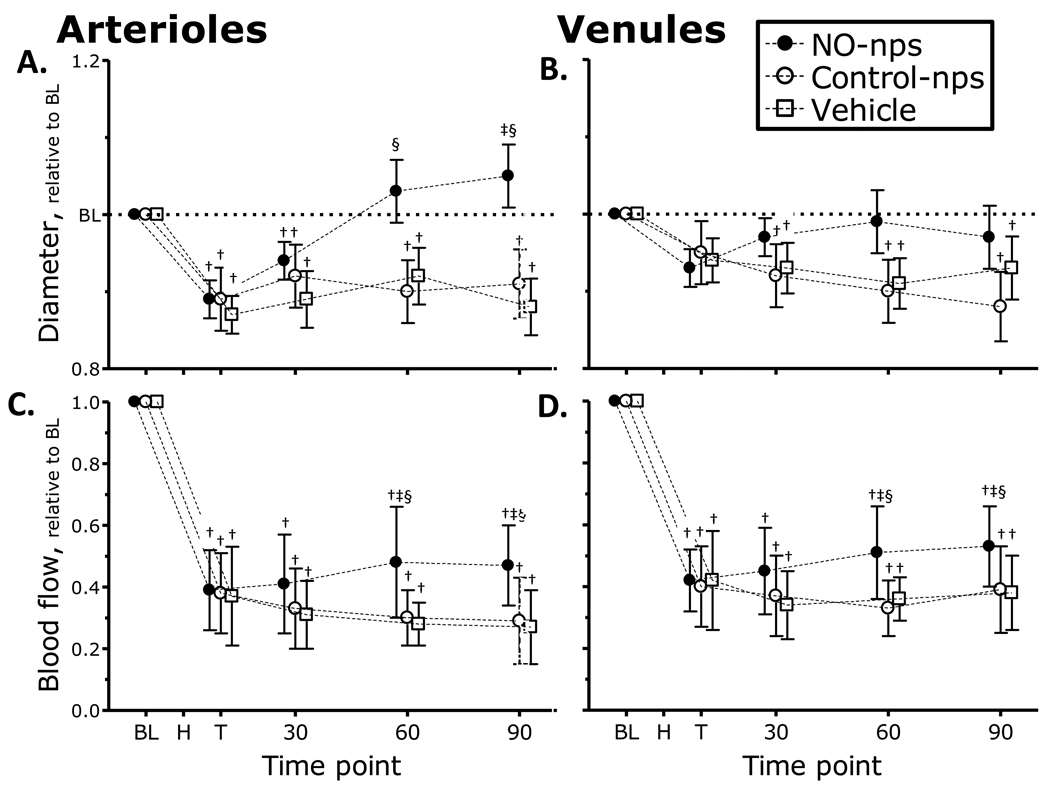
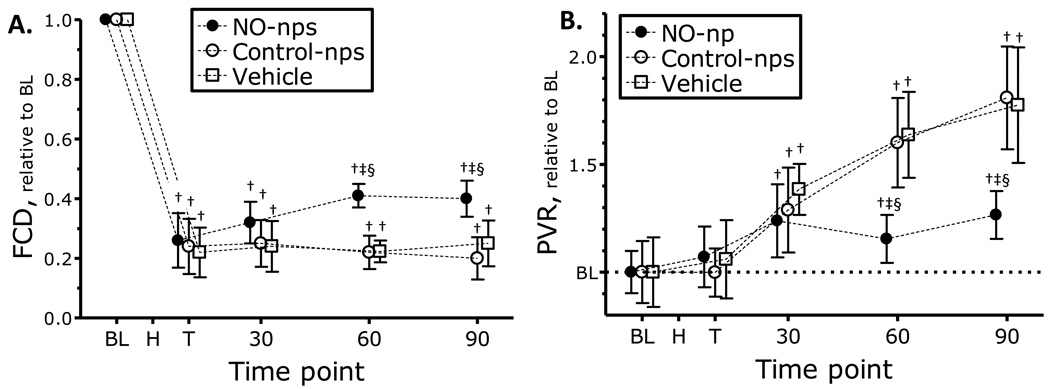
This study investigated the systemic and microvascular hemodynamic changes related to increased nitric oxide (NO) availability following significant hemorrhage, made available by administration of NO releasing nanoparticles (NO-nps). Hemodynamic responses to hemorrhagic shock were studied in the hamster window chamber. Acute hemorrhage was induced by arterial controlled bleeding of 50% of blood volume, and the resulting hemodynamic parameters were followed over 90 min. Exogenous NO was administered in the form of NO-nps (5mg/kg suspended in 50 μl saline) 10 min following induced hemorrhage. Control groups received equal dose of NO free nanoparticles (Control-nps) and Vehicle solution. Animals treated with NO-nps partially maintained systemic and microvascular function during hypovolemic shock compared to animals treated with Control-nps or the Vehicle (50 μl saline). The continuous NO released by the NO-nps reverted arteriolar vasoconstriction, partially recovered both functional capillary density and microvascular blood flows. Additionally, NO supplementation post hemorrhage prevented cardiac decompensation, and thereby maintained and stabilized the heart rate. Paradoxically, the peripheral vasodilation induced by the NO-nps did not decrease blood pressure, and combined with NO's effects on vascular resistance, NO-nps promoted intravascular pressure redistribution and blood flow, avoiding tissue ischemia. Therefore, by increasing NO availability with NO-nps during hypovolemic shock, it is possible that cardiac stability and microvascular perfusion can be preserved, ultimately increasing survivability and local tissue viability, and reducing hemorrhagic shock sequelae. The relevance, stability, and efficacy of exogenous NO therapy in the form of NO-nps will potentially facilitate the intended use in battlefield and trauma situations.
Copyright © 2011 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
No conflicts of interest to declare.
Figures
References
-
- Bellamy RF. The causes of death in conventional land warfare: implications for combat casualty care research. Mil Med. 1984;149:55–62. - PubMed
-
- Pope AM Institute of Medicine (U.S.) Fluid resuscitation : state of the science for treating combat casualties and civilian injuries. Washington, D.C.: National Academy Press; 1999. - PubMed
-
- Bacter CR, Canizaro PC, Carrico CJ, Shires GT. Fluid resuscitation of hemorrhagic shock. Postgrad Med. 1970;48:95–99. - PubMed
-
- Burris D, Rhee P, Kaufmann C, Pikoulis E, Austin B, Eror A, et al. Controlled resuscitation for uncontrolled hemorrhagic shock. J Trauma. 1999;46:216–223. - PubMed
-
- Dubick MA, Atkins JL. Small-volume fluid resuscitation for the far-forward combat environment: current concepts. J Trauma. 2003;54:S43–S45. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
