

Endotoxemia related to cardiopulmonary bypass is associated with increased risk of infection after cardiac surgery: a prospective observational study
- PMID: 21345192
- PMCID: PMC3222002
- DOI: 10.1186/cc10051
Endotoxemia related to cardiopulmonary bypass is associated with increased risk of infection after cardiac surgery: a prospective observational study
Abstract
Introduction: Previous studies have documented a high frequency of endotoxemia associated with cardiopulmonary bypass (CPB). Endotoxemia may be responsible for some of the complications associated with cardiac surgery. The purpose of the study was to examine the prevalence of endotoxemia during cardiopulmonary bypass supported aortocoronary bypass grafting surgery (ACB) using a new assay, the Endotoxin Activity Assay (EAA), and explore the association between endotoxemia and post-operative infection.
Methods: The study was a single center prospective observational study measuring EAA during the perioperative period for elective ACB. Blood samples were drawn at induction of anesthesia (T1), immediately prior to release of the aortic cross-clamp (T2), and on the first post-operative morning (T3). The primary outcome was the prevalence of endotoxemia. Secondary outcomes assessed included infection rates, intensive care unit (ICU) and hospital length of stay. An EAA of < 0.40 units was interpreted as "low", 0.41 to 0.59 units as "intermediate", and ≥ 0.60 units as "high".
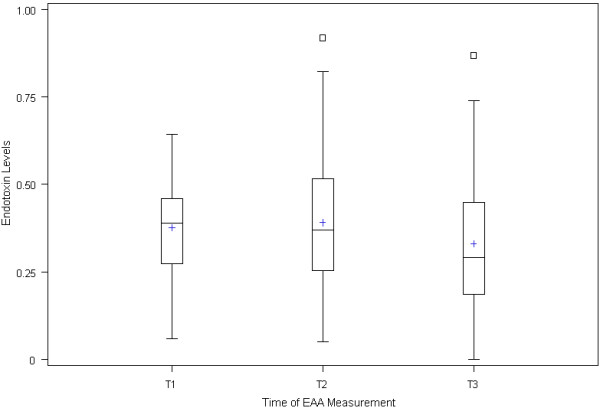
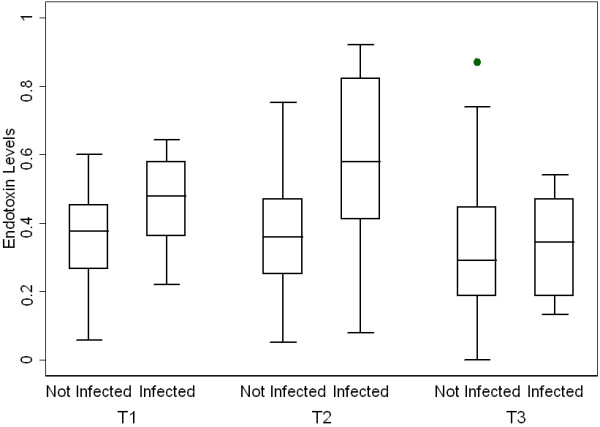
Results: A total of 57 patients were enrolled and 54 patients were analyzable. The mean EAA at T1 was 0.38 +/- 0.14, at T2 0.39 +/- 0.18, and at T3 0.33 +/- 0.18. At T2 only 13.5% (7/52) of patients had an EAA in the high range. There was a positive correlation between EAA and duration of surgery (P = 0.02). In patients with EAA ≥ 0.40 at T2, 26.1% (6/23) of patients developed post-operative infections compared to 3.5% (1/29) of those that had a normal EAA (P = 0.0354). Maximum EAA over the first 24 hours was also strongly correlated with risk of post-operative infection (P = 0.0276).
Conclusions: High levels of endotoxin occur less frequently during ACB than previously documented. However, endotoxemia is associated with a significantly increased risk of the development of post-operative infection. Measuring endotoxin levels during ACB may provide a mechanism to identify and target a high risk patient population.
Figures
References
-
- Antonelli M, Testa G, Tritapepe L, D'Errico RR, Costa D, Giovannelli L, Riccioni L, Gasparetto A, Catena G. IL-8, IL-6 and ICAM-1 in serum of paediatric patients undergoing cardiopulmonary bypass with and without cardiocirculatory arrest. J Cardiovasc Surg (Torino) 1999;40:803–809. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
