

Temozolomide in the treatment of children with newly diagnosed diffuse intrinsic pontine gliomas: a report from the Children's Oncology Group
- PMID: 21345842
- PMCID: PMC3064697
- DOI: 10.1093/neuonc/noq205
Temozolomide in the treatment of children with newly diagnosed diffuse intrinsic pontine gliomas: a report from the Children's Oncology Group
Abstract
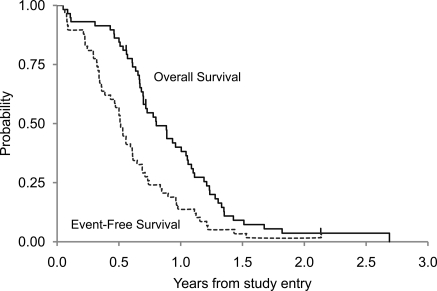
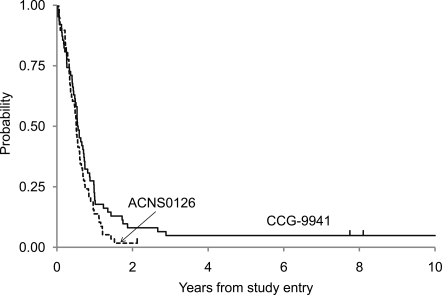
An open-label phase II study (ACNS0126) testing the efficacy of chemoradiotherapy with temozolomide (TMZ) followed by adjuvant TMZ was conducted by the Children's Oncology Group. During the period from July 6, 2004 through September 6, 2005, 63 children with newly diagnosed diffuse intrinsic pontine glioma (DIPG) were enrolled in the study. All patients received TMZ at a dosage of 90 mg/m(2)/day for 42 days to a dose of 59.4 Gy. Four weeks following irradiation, TMZ was given at a dosage of 200 mg/m(2)/day for 5 days every 28 days, for a total of 10 cycles. The primary objective of the statistical analysis was to determine whether the current treatment produced a 1-year event-free survival (EFS) rate higher than the historical baseline of 21.9% observed in CCG-9941. The mean 1-year EFS (± standard deviation) was 14% ± 4.5%, compared with 21.9% ± 5% for CCG-9941. The P value of the test of comparison of 1-year EFS, based on a 1-sided, 1-sample test of proportions, was .96. There was no evidence that temozolomide produced a 1-year EFS rate higher than 21.9%. The mean 1-year OS (± standard deviation) was 40% ± 6.5%, compared with 32% ± 6% for CCG-9941. The median time to death was 9.6 months. Chemoradiotherapy with TMZ followed by adjuvant TMZ is not more effective than previously reported regimens for the treatment of children with DIPG.
Figures
References
-
- Donaldson SS, Laningham F, Fisher PG. Advances toward an understanding of brainstem gliomas. J Clin Oncol. 2006;24(8):1266–1272. - PubMed
-
- Schumacher M, Schulte-Monting J, Stoeter P, et al. Magnetic resonance imaging compared with biopsy in the diagnosis of brainstem diseases of childhood: a multicenter review. J Neurosurg. 2007;106(2 Suppl):111–119. - PubMed
-
- Hargrave D, Bartels U, Bouffet E. Diffuse brainstem glioma in children: critical review of clinical trials. Lancet Oncol. 2006;7(3):241–248. - PubMed
-
- Laigle-Donadey F, Doz F, Delattre JY. Brainstem gliomas in children and adults. Curr Opin Oncol. 2008;20(6):662–667. - PubMed
-
- Langmoen IA, Lundar T, Storm-Mathisen I, et al. Management of pediatric pontine gliomas. Childs Nerv Syst. 1991;7(1):13–15. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
