

Influence of individual brightness and contrast adjustment on accuracy of radiographic measurements of infrabony defects
- PMID: 21346085
- PMCID: PMC3611457
- DOI: 10.1259/dmfr/56018062
Influence of individual brightness and contrast adjustment on accuracy of radiographic measurements of infrabony defects
Abstract
Objectives: To assess the accuracy of radiographic measurements of infrabony defects and to compare the accuracy with and without individual digital adjustment of brightness and contrast.
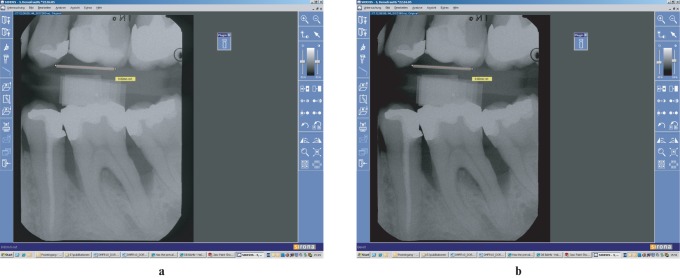
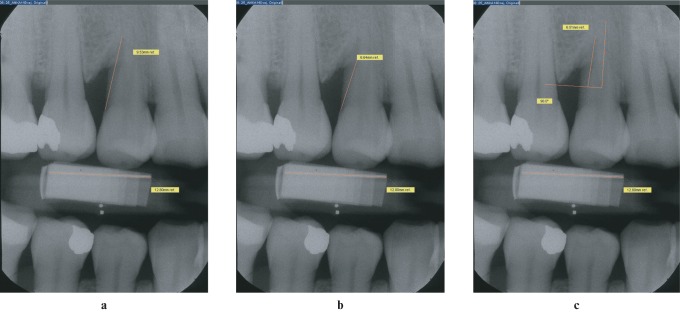
Methods: In 41 periodontitis patients (19 females, 22 males; age range 23-73 years), 50 radiographs of 50 infrabony defects were obtained. All radiographs were digitized. Using a personal computer program, the linear distances between cemento-enamel junction (CEJ) and alveolar crest (AC) and between CEJ and bony defect (BD), and the depth of the infrabony defect (INFRA), were measured twice, according to the individual judgement of the radiographic examiner: (1) without digital adjustment (W) and (2) after use of contrast and brightness adjustment (A). Intrasurgical bone measurements served as the gold standard. The accuracy of measurements with or without digital adjustment was compared.
Results: Radiographic measurements underestimated the gold standard for CEJ-BD (W: 1.1 mm ± 1.8 mm, P < 0.001; A: 1.0 mm ± 1.9 mm, P = 0.001). Both CEJ-AC (W: 0.2 mm ± 2.5 mm; A: 0.5 mm ± 2.6 mm) and INFRA (W: -0.4 mm ± 2.4 mm; A: -0.6 mm ± 2.5 mm) measurements came close to the gold standard. Statistically significant differences between W and A regarding accuracy were not observed.
Conclusions: The measurement tool used in this study provided high-accuracy measurements of periodontal bone loss in INFRA. Individual brightness and contrast adjustment failed to improve accuracy.
Figures
References
-
- Tonetti MS, Pini Prato G, Williams RC, Cortellini P. Periodontal regeneration of human infrabony defects. III. Diagnostic strategies to detect bone gain. J Periodontol 1993;64:269–277 - PubMed
-
- Klein F, Kim T-S, Hassfeld S, Staehle HJ, Reitmeir P, Holle R, et al. Radiographic defect depth and width for prognosis and description of periodontal healing of infrabony defects. J Periodontol 2001;72:1639–1646 - PubMed
-
- Eickholz P, Hörr T, Klein F, Hassfeld S, Kim T-S. Radiographic parameters for prognosis of periodontal healing of infrabony defects: Two different definitions of defect depth. J Periodontol 2004;75:399–407 - PubMed
-
- Theilade J. An evaluation of the reliability of radiographs in the measurement of bone loss in periodontal disease. J Periodontol 1960;31:143–153
-
- Suomi JD, Plumbo J, Barbano JP. A comparative study of radiographs and pocket measurements in periodontal disease evaluation. J Periodontol 1968;39:311–315 - PubMed
