

Defining hematoma expansion in intracerebral hemorrhage: relationship with patient outcomes
- PMID: 21346218
- PMCID: PMC3068004
- DOI: 10.1212/WNL.0b013e3182143317
Defining hematoma expansion in intracerebral hemorrhage: relationship with patient outcomes
Abstract
Background: Hematoma expansion (HE) is a surrogate marker in intracerebral hemorrhage (ICH) trials. However, the amount of HE necessary to produce poor outcomes in an individual is unclear; there is no agreement on a clinically meaningful definition of HE. We compared commonly used definitions of HE in their ability to predict poor outcome as defined by various cutpoints on the modified Rankin Scale (mRS).
Methods: In this cohort study, we analyzed 531 patients with ICH from the Virtual International Stroke Trials Archive. Primary outcome was mRS at 90 days, dichotomized into 0-3 vs 4-6. Secondary outcomes included other mRS cutpoints and mRS "shift analysis." Sensitivity, specificity, and predictive values for commonly used HE definitions were calculated.
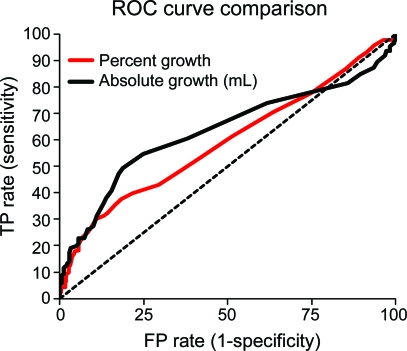
Results: Between 13% and 32% of patients met the commonly used HE definitions. All definitions independently predicted poor outcome; positive predictive values increased with higher growth cutoffs but at the expense of lower sensitivities. All HE definitions showed higher specificity than sensitivity. Absolute growth cutoffs were more predictive than relative cutoffs when mRS 5-6 or 6 was defined as "poor outcome."
Conclusion: HE robustly predicts poor outcome regardless of the growth definition or the outcome definition. The highest positive predictive values are obtained when using an absolute growth definition to predict more severe outcomes. Given that only a minority of patients may have clinically relevant HE, hemostatic ICH trials may need to enroll a large number of patients, or select for a population that is more likely to have HE.
Figures
Comment in
-
Intracerebral hematoma expansion: making predictions (about the future).Neurology. 2011 Apr 5;76(14):1204-5. doi: 10.1212/WNL.0b013e31821435d0. Epub 2011 Feb 23. Neurology. 2011. PMID: 21346224 No abstract available.
References
-
- Rost NS, Smith EE, Chang Y, et al. Prediction of functional outcome in patients with primary intracerebral hemorrhage: the FUNC score. Stroke 2008;39:2304–2309 - PubMed
-
- van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol 2010;9:167–176 - PubMed
-
- Kazui S, Naritomi H, Yamamoto H, Sawada T, Yamaguchi T. Enlargement of spontaneous intracerebral hemorrhage: incidence and time course. Stroke 1996;27:1783–1787 - PubMed
-
- Davis SM, Broderick J, Hennerici M, et al. , Recombinant Activated Factor VII Intracerebral Hemorrhage Trial Investigators Hematoma growth is a determinant of mortality and poor outcome after intracerebral hemorrhage. Neurology 2006;66:1175–1181 - PubMed
-
- Demchuk AM, Kosior J, Tymchuk S, et al. Multicentre prospective study demonstrates validity of CTA spot sign for hematoma expansion prediction in noncoagulopathic primary ICH patients. Cerebrovasc Dis 2008;25 (suppl 2):52
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous