

The intact nephron hypothesis: the concept and its implications for phosphate management in CKD-related mineral and bone disorder
- PMID: 21346721
- PMCID: PMC3260962
- DOI: 10.1038/ki.2011.23
The intact nephron hypothesis: the concept and its implications for phosphate management in CKD-related mineral and bone disorder
Abstract
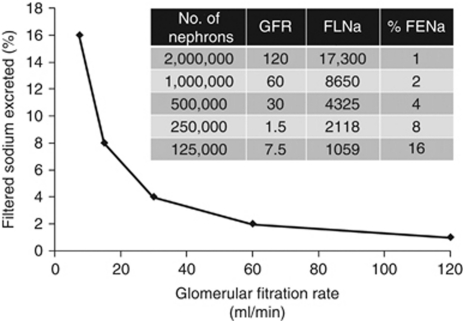
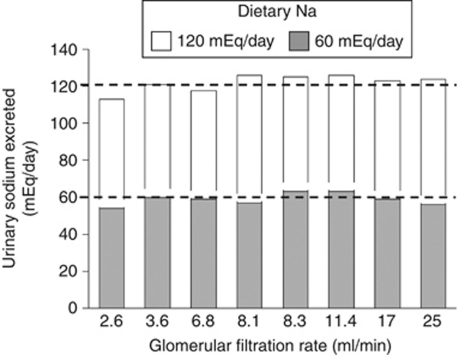
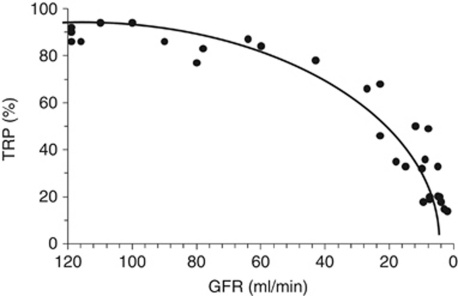
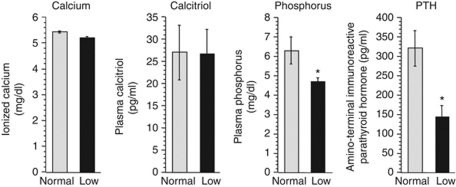
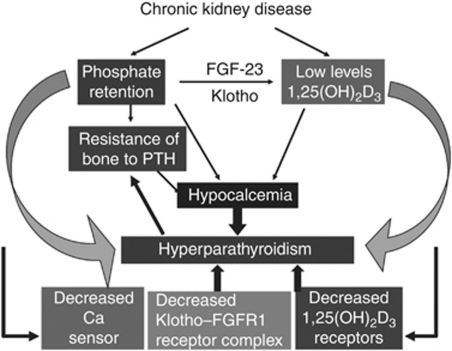
Mechanistic understanding of secondary hyperparathyroidism, vascular calcification, and regulation of phosphate metabolism in chronic kidney disease (CKD) has advanced significantly in the past five decades. In 1960, Bricker developed the 'intact nephron hypothesis', opening the door for hundreds of investigations. He emphasized that 'as the number of functioning nephrons decreases, each remaining nephron must perform a greater fraction of total renal excretion'. Phosphate per se, independent of Ca²+ and calcitriol, directly affects the development of parathyroid gland hyperplasia and secondary hyperparathyroidism. Vitamin D receptor, Ca²+ sensing receptor, and Klotho-fibroblast growth factor (FGF) receptor-1 complex are all significantly decreased in the parathyroid glands of patients with CKD. Duodenal instillation of phosphate rapidly decreases parathyroid hormone release without changes in calcium or calcitriol. The same procedure also rapidly increases renal phosphate excretion independently of FGF-23, suggesting the possibility of an 'intestinal phosphatonin'. These observations suggest a possible 'phosphate sensor' in the parathyroid glands and gastrointestinal tract, although as yet there is no proof for the existence of such a sensor. Evidence shows that phosphate has a key role in parathyroid hyperplasia by activating the transforming growth factor-α-epidermal growth factor receptor complex. Thus, control of serum phosphorus early in the course of CKD will significantly ameliorate the pathological manifestations observed during progressive deterioration of renal function.
Figures

Similar articles
-
The intact nephron hypothesis: the concept and its implications for phosphate management in CKD-related mineral and bone disorder.Kidney Int. 2011 Apr;79121:S3-8. doi: 10.1038/ki.2011.23. Kidney Int. 2011. PMID: 26746859 Review.
-
[Changes in mineral metabolism in stage 3, 4, and 5 chronic kidney disease (not on dialysis)].Nefrologia. 2008;28 Suppl 3:67-78. Nefrologia. 2008. PMID: 19018742 Spanish.
-
Connections between vascular calcification and progression of chronic kidney disease: therapeutic alternatives.Kidney Int Suppl. 2005 Dec;(99):S142-51. doi: 10.1111/j.1523-1755.2005.09926.x. Kidney Int Suppl. 2005. PMID: 16336568
-
What would we like to know, and what do we not know about fibroblast growth factor 23?J Nephrol. 2011 Nov-Dec;24(6):696-706. doi: 10.5301/jn.5000003. J Nephrol. 2011. PMID: 21786227 Review.
-
Phosphate and FGF-23.Kidney Int Suppl. 2011 Apr;79(121):S24-7. doi: 10.1038/ki.2011.27. Epub 2011 Feb 23. Kidney Int Suppl. 2011. PMID: 21346724 Free PMC article. Review.
Cited by
-
Urinary phosphorus excretion per creatinine clearance as a prognostic marker for progression of chronic kidney disease: a retrospective cohort study.BMC Nephrol. 2015 Jul 28;16:116. doi: 10.1186/s12882-015-0118-1. BMC Nephrol. 2015. PMID: 26215643 Free PMC article.
-
Decreased renal function increases the nighttime urine volume rate by carryover of salt excretion to the nighttime.Sci Rep. 2021 May 19;11(1):10587. doi: 10.1038/s41598-021-90166-x. Sci Rep. 2021. PMID: 34012017 Free PMC article.
-
A Shared Nephroprotective Mechanism for Renin-Angiotensin-System Inhibitors, Sodium-Glucose Co-Transporter 2 Inhibitors, and Vasopressin Receptor Antagonists: Immunology Meets Hemodynamics.Int J Mol Sci. 2022 Apr 1;23(7):3915. doi: 10.3390/ijms23073915. Int J Mol Sci. 2022. PMID: 35409276 Free PMC article. Review.
-
Prognostic importance of plasma total magnesium in a cohort of cats with azotemic chronic kidney disease.J Vet Intern Med. 2018 Jul;32(4):1359-1371. doi: 10.1111/jvim.15141. Epub 2018 Apr 27. J Vet Intern Med. 2018. PMID: 29704284 Free PMC article.
-
Fibroblast growth factor 23 and symmetric dimethylarginine concentrations in geriatric cats.J Vet Intern Med. 2019 Nov;33(6):2657-2664. doi: 10.1111/jvim.15590. Epub 2019 Sep 30. J Vet Intern Med. 2019. PMID: 31568615 Free PMC article.
References
-
- Bricker NS, Morrin PA, Kime SW., Jr The pathologic physiology of chronic Bright's disease. An exposition of the ‘intact nephron hypothesis'. Am J Med. 1960;28:77–98. - PubMed
-
- Bricker NS. On the pathogenesis of the uremic state. An exposition of the ‘trade-off hypothesis'. N Engl J Med. 1972;286:1093–1099. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
