

Cardiac output in idiopathic normal pressure hydrocephalus: association with arterial blood pressure and intracranial pressure wave amplitudes and outcome of shunt surgery
- PMID: 21349148
- PMCID: PMC3044095
- DOI: 10.1186/2045-8118-8-11
Cardiac output in idiopathic normal pressure hydrocephalus: association with arterial blood pressure and intracranial pressure wave amplitudes and outcome of shunt surgery
Abstract
Background: In patients with idiopathic normal pressure hydrocephalus (iNPH) responding to shunt surgery, we have consistently found elevated intracranial pressure (ICP) wave amplitudes during diagnostic ICP monitoring prior to surgery. It remains unknown why ICP wave amplitudes are increased in these patients. Since iNPH is accompanied by a high incidence of vascular co-morbidity, a possible explanation is that there is reduced vascular compliance accompanied by elevated arterial blood pressure (ABP) wave amplitudes and even altered cardiac output (CO). To investigate this possibility, the present study was undertaken to continuously monitor CO to determine if it is correlated to ABP and ICP wave amplitudes and the outcome of shunting in iNPH patients. It was specifically addressed whether the increased ICP wave amplitudes seen in iNPH shunt responders were accompanied by elevated CO and/or ABP wave amplitude levels.
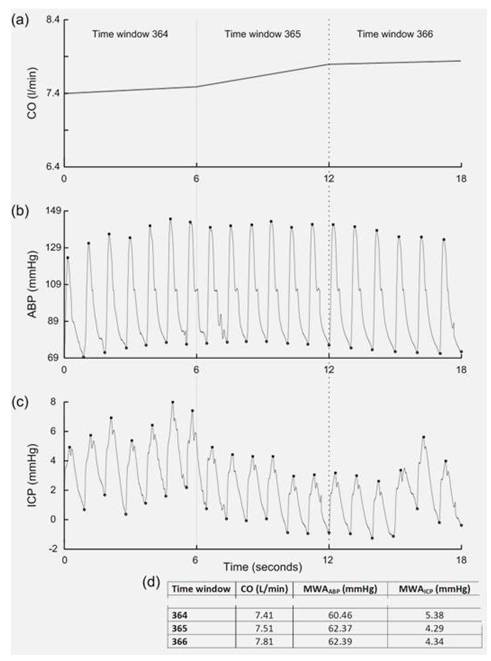
Methods: Prospective iNPH patients (29) were clinically graded using an NPH grading scale. Continuous overnight minimally-invasive monitoring of CO and ABP was done simultaneously with ICP monitoring; the CO, ABP, and ICP parameters were parsed into 6-second time windows. Patients were assessed for shunt surgery on clinical grade, Evan's index, and ICP wave amplitude. Follow-up clinical grading was performed 12 months after surgery.
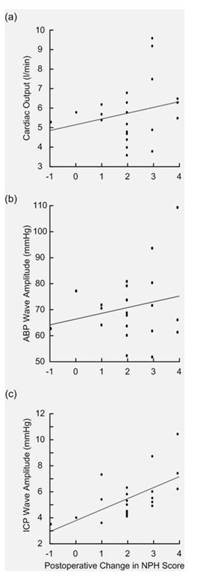
Results: ICP wave amplitudes but not CO or ABP wave amplitude, showed good correlation with the response to shunt treatment. The patients with high ICP wave amplitude did not have accompanying high levels of CO or ABP wave amplitude. Correlation analysis between CO and ICP wave amplitudes in individual patients showed different profiles [significantly positive in 10 (35%) and significantly negative in 16 (55%) of 29 recordings]. This depended on whether there was also a correlation between ABP and ICP wave amplitudes and on the average level of ICP wave amplitude.
Conclusions: These results gave no evidence that the increased levels of ICP wave amplitudes seen in iNPH shunt responders prior to surgery were accompanied by elevated levels of ABP wave amplitudes or elevated CO. In the individual patients the correlation between CO and ICP wave amplitude was partly related to an association between ABP and ICP wave amplitudes which can be indicative of the state of cerebrovascular pressure regulation, and partly related to the ICP wave amplitude which can be indicative of the intracranial compliance.
Figures
Similar articles
-
Intracranial pulse pressure amplitude levels determined during preoperative assessment of subjects with possible idiopathic normal pressure hydrocephalus.Acta Neurochir (Wien). 2006 Nov;148(11):1151-6; discussion 1156. doi: 10.1007/s00701-006-0896-0. Epub 2006 Oct 16. Acta Neurochir (Wien). 2006. PMID: 17039303
-
Cerebrospinal fluid pulse pressure amplitude during lumbar infusion in idiopathic normal pressure hydrocephalus can predict response to shunting.Cerebrospinal Fluid Res. 2010 Feb 12;7:5. doi: 10.1186/1743-8454-7-5. Cerebrospinal Fluid Res. 2010. PMID: 20205911 Free PMC article.
-
Mechanisms behind altered pulsatile intracranial pressure in idiopathic normal pressure hydrocephalus: role of vascular pulsatility and systemic hemodynamic variables.Acta Neurochir (Wien). 2020 Aug;162(8):1803-1813. doi: 10.1007/s00701-020-04423-5. Epub 2020 Jun 12. Acta Neurochir (Wien). 2020. PMID: 32533412 Free PMC article.
-
Diagnostic intracranial pressure monitoring and surgical management in idiopathic normal pressure hydrocephalus: a 6-year review of 214 patients.Neurosurgery. 2010 Jan;66(1):80-91. doi: 10.1227/01.NEU.0000363408.69856.B8. Neurosurgery. 2010. PMID: 20023540 Review.
-
Risk factors, comorbidities, quality of life, and complications after surgery in idiopathic normal pressure hydrocephalus: review of the INPH-CRasH study.Neurosurg Focus. 2020 Oct;49(4):E8. doi: 10.3171/2020.7.FOCUS20466. Neurosurg Focus. 2020. PMID: 33002861 Review.
Cited by
-
Cerebral Haemodynamics: Effects of Systemic Arterial Pulsatile Function and Hypertension.Curr Hypertens Rep. 2018 Mar 19;20(3):20. doi: 10.1007/s11906-018-0822-x. Curr Hypertens Rep. 2018. PMID: 29556793 Review.
-
Cerebrospinal fluid and venous biomarkers of shunt-responsive idiopathic normal pressure hydrocephalus: a systematic review and meta-analysis.Acta Neurochir (Wien). 2022 Jul;164(7):1719-1746. doi: 10.1007/s00701-022-05154-5. Epub 2022 Mar 1. Acta Neurochir (Wien). 2022. PMID: 35230552 Free PMC article.
-
Measuring intracranial pressure by invasive, less invasive or non-invasive means: limitations and avenues for improvement.Fluids Barriers CNS. 2020 May 6;17(1):34. doi: 10.1186/s12987-020-00195-3. Fluids Barriers CNS. 2020. PMID: 32375853 Free PMC article. Review.
-
Continuous wavelet transform in the study of the time-scale properties of intracranial pressure in hydrocephalus.Philos Trans A Math Phys Eng Sci. 2018 Aug 13;376(2126):20170251. doi: 10.1098/rsta.2017.0251. Philos Trans A Math Phys Eng Sci. 2018. PMID: 29986920 Free PMC article.
-
Clinical predictors of shunt response in the diagnosis and treatment of idiopathic normal pressure hydrocephalus: a systematic review and meta-analysis.Acta Neurochir (Wien). 2021 Oct;163(10):2641-2672. doi: 10.1007/s00701-021-04922-z. Epub 2021 Jul 8. Acta Neurochir (Wien). 2021. PMID: 34235589 Free PMC article.
References
LinkOut - more resources
Full Text Sources
