

The relative atrial volume ratio and late gadolinium enhancement provide additive information to differentiate constrictive pericarditis from restrictive cardiomyopathy
- PMID: 21349202
- PMCID: PMC3058035
- DOI: 10.1186/1532-429X-13-15
The relative atrial volume ratio and late gadolinium enhancement provide additive information to differentiate constrictive pericarditis from restrictive cardiomyopathy
Abstract
Background: The differentiation of constrictive pericarditis (CP) from restrictive cardiomyopathy (RCM) is often difficult. This study sought to determine the clinical utility of cardiovascular magnetic resonance imaging (CMR) for differentiating both these disorders.
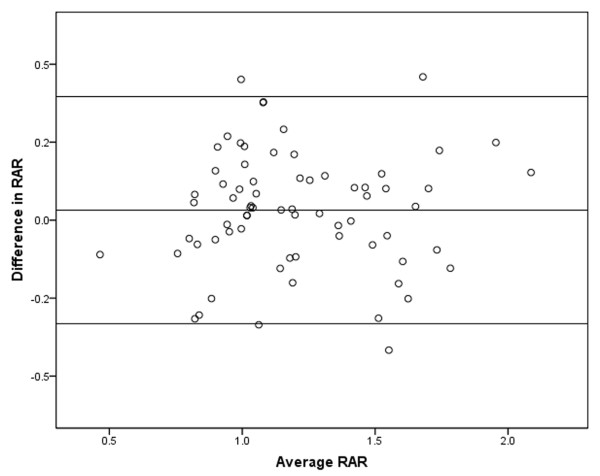
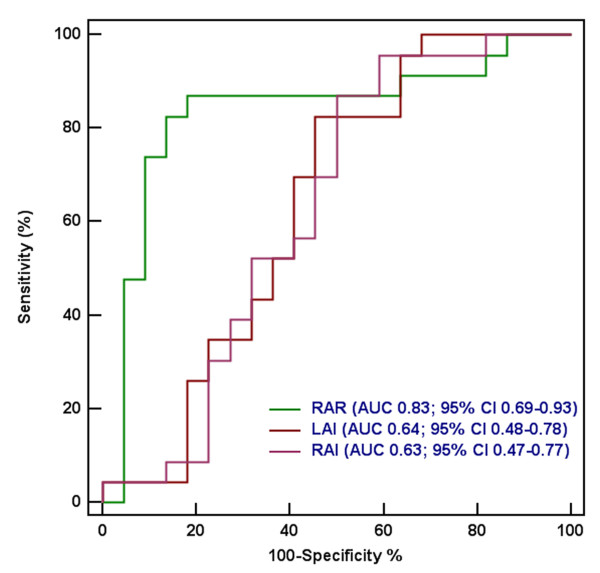
Methods: Twenty-three patients with surgically documented CP, 22 patients with RCM and 25 normal subjects were included in the study. CMR yielded information about cardiac morphology, function and tissue characteristics. The left (LA) and right atrial (RA) volume was calculated using the area-length method. The relative atrial volume ratio (RAR) was defined as the LA volume divided by RA volume. Receiver operating characteristic curve analysis was used to test the ability of different variables in differentiating CP from RCM.
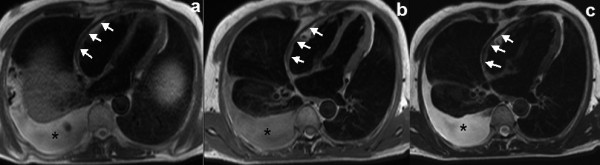
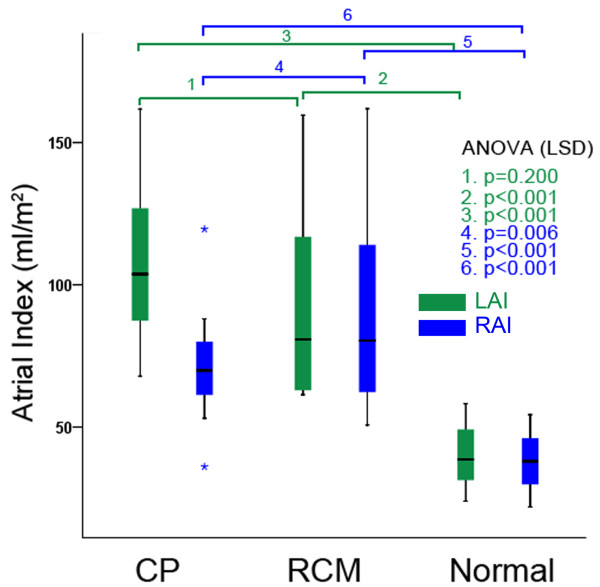
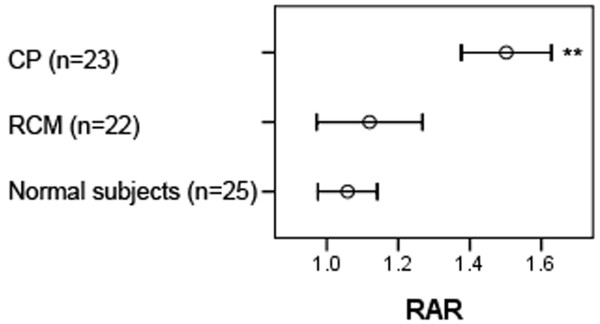
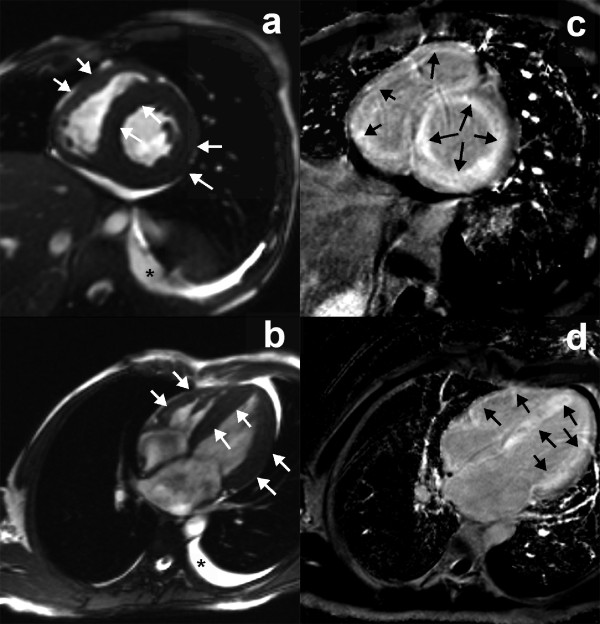
Results: The maximal pericardial thickness in CP patients was significantly larger than in normal subjects and RCM patients. The RA volume index in RCM patients (90.5 ± 35.3 mL/m2) was significantly larger than in CP patients (71.4 ± 15.7 mL/m2, p = 0.006) and normal subjects (38.1 ± 9.0 mL/m2, p < 0.001). The LA volume index in RCM (96.0 ± 37.0 mL/m2) and CP patients (105.6 ± 25.1 mL/m2) was significantly larger than in normal subjects (39.5 ± 9.5 mL/m2, p < 0.001 for all). The RAR in CP patients (1.50 ± 0.29) was significantly larger than in RCM patients (1.12 ± 0.33, p < 0.001) and normal subjects (1.06 ± 0.20, p < 0.001). There were no differences between RCM patients and normal subjects in the RAR (p = 0.452). At a cut-off value of 1.32 for the RAR, the sensitivity was 82.6%, and the specificity was 86.4% in the detection of CP. Septal bounce was identified in 95.7% CP patients, in none of RCM patients and normal subjects. Late gadolinium enhancement (LGE) was present in 31.8% RCM patients and absence in all CP patients and normal subjects.
Conclusions: CMR with LGE and RAR can facilitate differentiation of CP from RCM.
Figures
References
-
- Bograd AJ, Mital S, Schwarzenberger JC, Mosca RS, Quaegebeur JM, Addonizio LJ, Hsu DT, Lamour JM, Chen JM. Twenty-year experience with heart transplantation for infants and children with restrictive cardiomyopathy: 1986-2006. Am J Transplant. 2008;8:201–207. - PubMed
-
- Ammash NM, Seward JB, Bailey KR, Edwards WD, Tajik AJ. Clinical profile and outcome of idiopathic restrictive cardiomyopathy. Circulation. 2000;101:2490–2496. - PubMed
-
- Talreja DR, Nishimura RA, Oh JK, Holmes DR. Constrictive pericarditis in the modern era: novel criteria for diagnosis in the cardiac catheterization laboratory. J Am Coll Cardiol. 2008;51:315–319. - PubMed
-
- Hurrell DG, Nishimura RA, Higano ST, Appleton CP, Danielson GK, Holmes DR Jr, Tajik AJ. Value of dynamic respiratory changes in left and right ventricular pressures for the diagnosis of constrictive pericarditis. Circulation. 1996;93:2007–2013. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
