

Management of ischemic optic neuropathies
- PMID: 21350282
- PMCID: PMC3116541
- DOI: 10.4103/0301-4738.77024
Management of ischemic optic neuropathies
Abstract
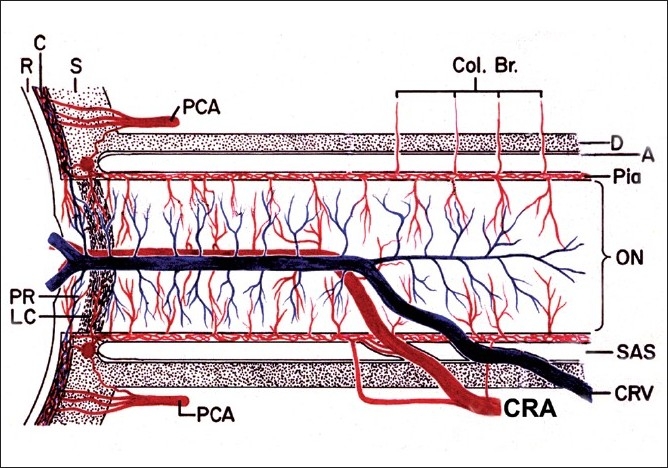
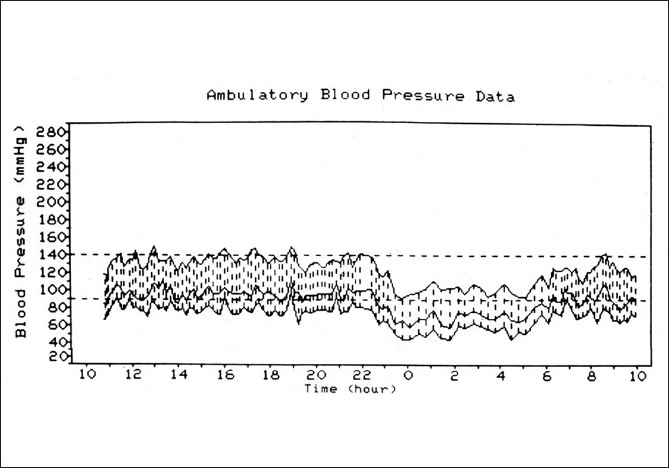
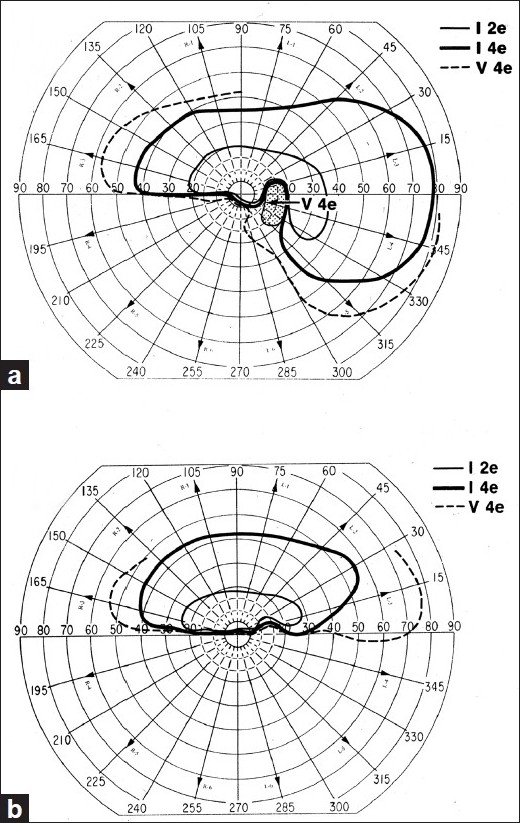
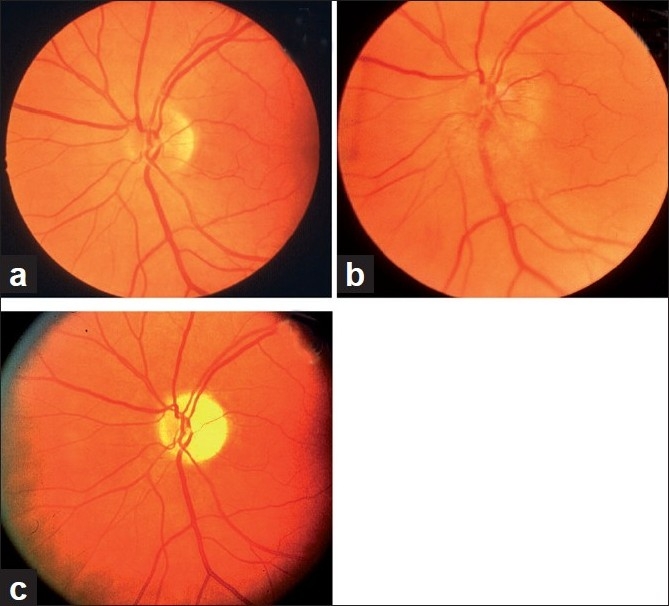
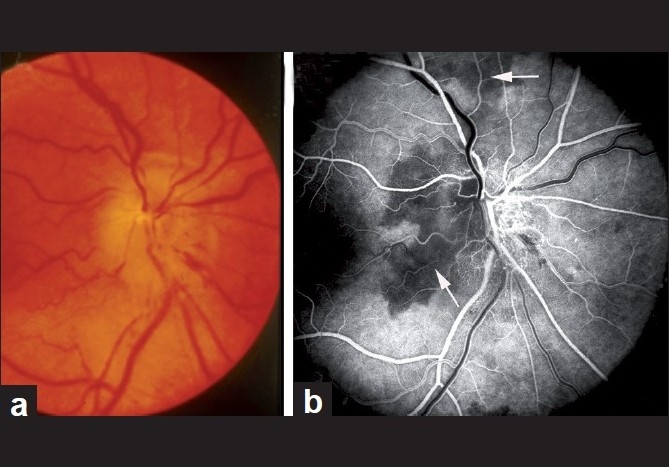
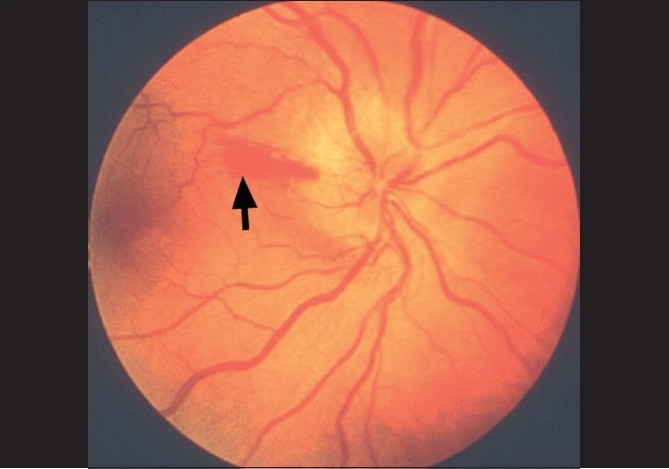
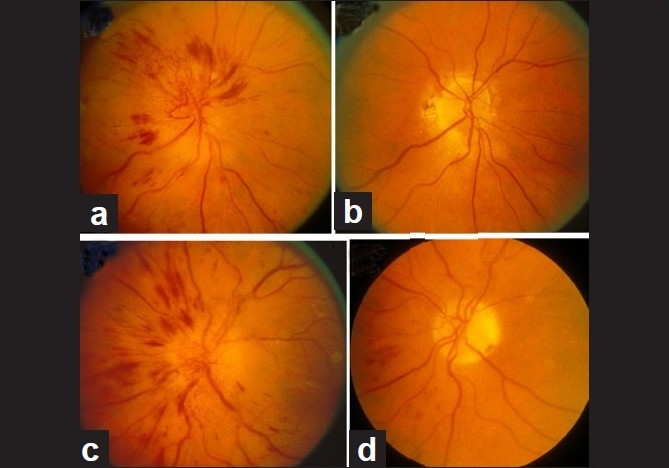
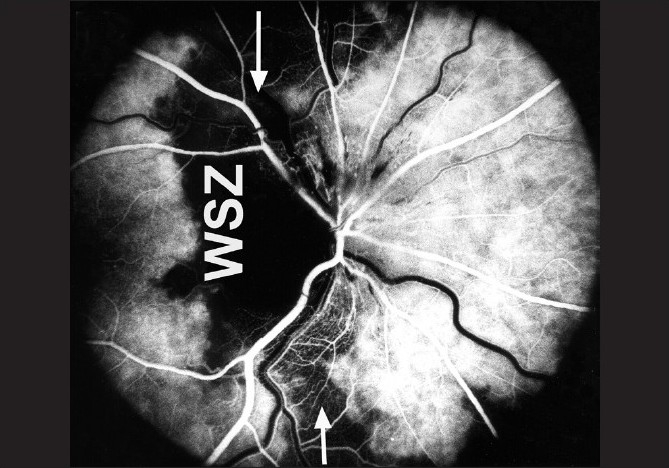
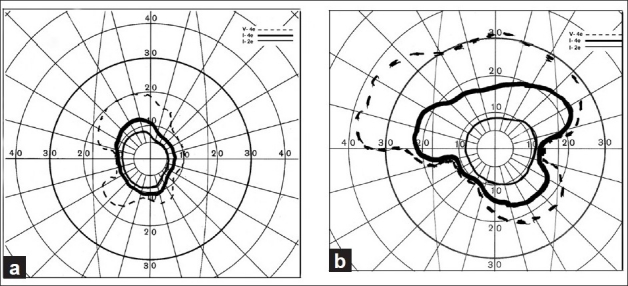
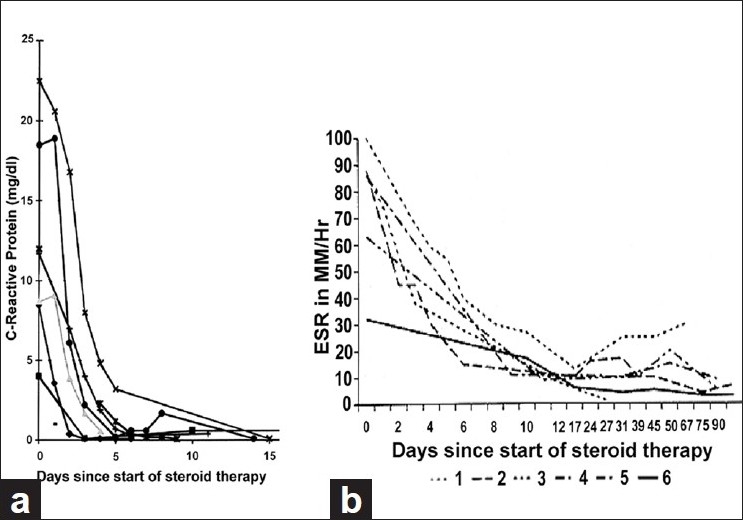
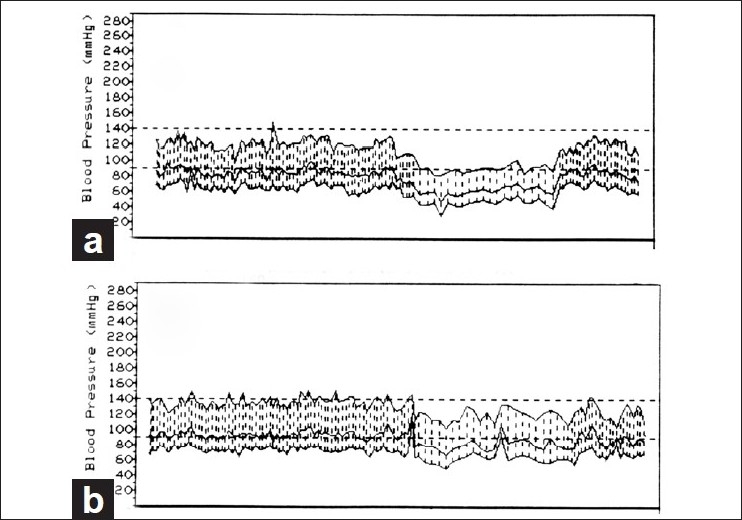
Ischemic optic neuropathies (IONs) consist primarily of two types: anterior ischemic optic neuropathy (AION) and posterior ischemic optic neuropathy (PION). AION comprises arteritic AION (A-AION: due to giant cell arteritis) and non-arteritic AION (NA-AION: due to other causes). PION consists of arteritic PION (A-PION: due to giant cell arteritis), non-arteritic PION (NA-PION: due to other causes), and surgical PION (a complication of several systemic surgical procedures). These five types of ION are distinct clinical entities etiologically, pathogenetically, clinically and from the management point of view. In the management of AION, the first crucial step with patients aged 50 and over is to identify immediately whether it is arteritic or not because A-AION is an ophthalmic emergency and requires urgent treatment with high-dose steroid therapy to prevent any further visual loss in one or both eyes. Patients with NA-AION, when treated with systemic corticosteroid therapy within first 2 weeks of onset, had significantly better visual outcome than untreated ones. Systemic risk factors, particularly nocturnal arterial hypotension, play major roles in the development of NA-AION; management of them is essential in its prevention and management. NA-PION patients, when treated with high-dose systemic steroid therapy during the very early stages of the disease, showed significant improvement in visual acuity and visual fields, compared to untreated eyes. A-PION, like A-AION, requires urgent treatment with high-dose steroid therapy to prevent any further visual loss in one or both eyes. There is no satisfactory treatment for surgical PION, except to take prophylactic measures to prevent its development.
Conflict of interest statement
Figures

References
-
- Hayreh SS. Anterior ischemic optic neuropathy. Heidelberg: Springer-Verlag; 1975.
-
- Hayreh SS. Blood supply and vascular disorders of the optic nerve. An Inst Barraquer. 1963;4:7–109.
-
- Hayreh SS. The 1994 Von Sallman lecture. The optic nerve head circulation in health and disease. Exp Eye Res. 1995;61:259–72. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
