

WHO absolute fracture risk models (FRAX): do clinical risk factors improve fracture prediction in older women without osteoporosis?
- PMID: 21351144
- PMCID: PMC3622725
- DOI: 10.1002/jbmr.372
WHO absolute fracture risk models (FRAX): do clinical risk factors improve fracture prediction in older women without osteoporosis?
Abstract
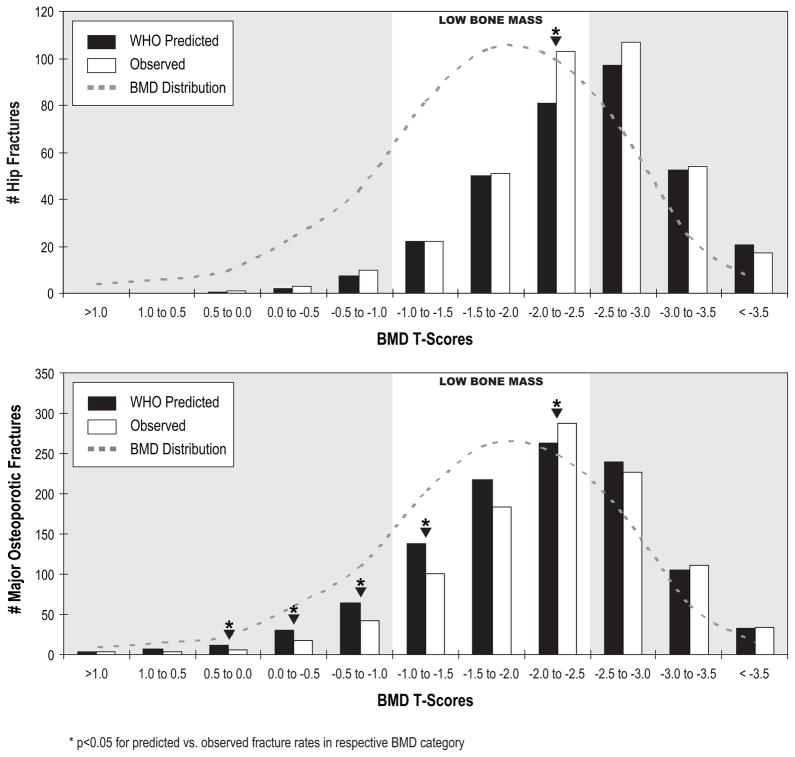
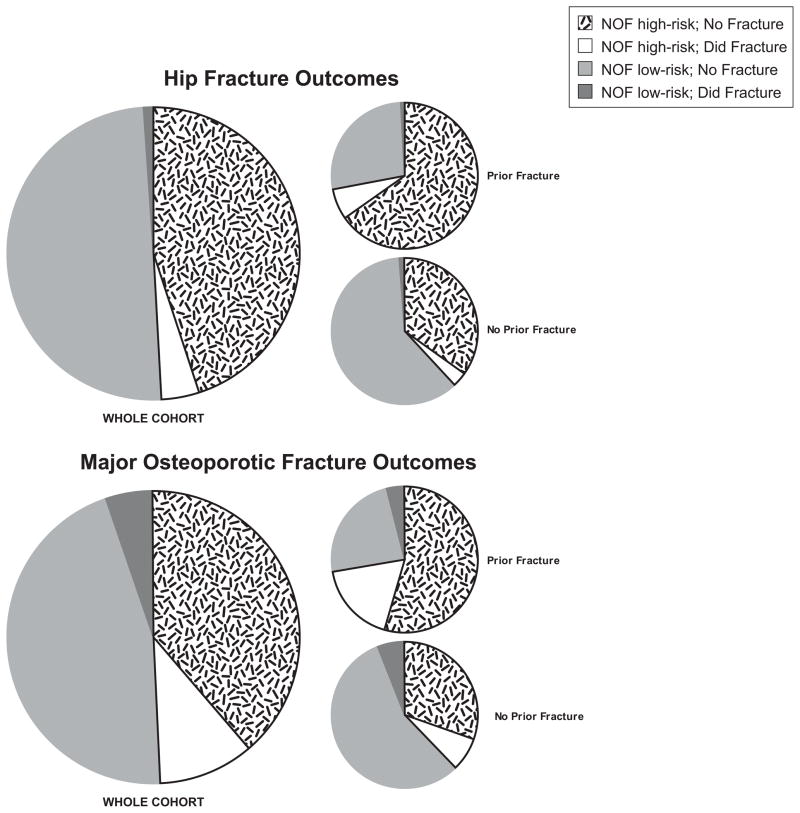
Bone mineral density (BMD) is a strong predictor of fracture, yet most fractures occur in women without osteoporosis by BMD criteria. To improve fracture risk prediction, the World Health Organization recently developed a country-specific fracture risk index of clinical risk factors (FRAX) that estimates 10-year probabilities of hip and major osteoporotic fracture. Within differing baseline BMD categories, we evaluated 6252 women aged 65 or older in the Study of Osteoporotic Fractures using FRAX 10-year probabilities of hip and major osteoporotic fracture (ie, hip, clinical spine, wrist, and humerus) compared with incidence of fractures over 10 years of follow-up. Overall ability of FRAX to predict fracture risk based on initial BMD T-score categories (normal, low bone mass, and osteoporosis) was evaluated with receiver-operating-characteristic (ROC) analyses using area under the curve (AUC). Over 10 years of follow-up, 368 women incurred a hip fracture, and 1011 a major osteoporotic fracture. Women with low bone mass represented the majority (n = 3791, 61%); they developed many hip (n = 176, 48%) and major osteoporotic fractures (n = 569, 56%). Among women with normal and low bone mass, FRAX (including BMD) was an overall better predictor of hip fracture risk (AUC = 0.78 and 0.70, respectively) than major osteoporotic fractures (AUC = 0.64 and 0.62). Simpler models (eg, age + prior fracture) had similar AUCs to FRAX, including among women for whom primary prevention is sought (no prior fracture or osteoporosis by BMD). The FRAX and simpler models predict 10-year risk of incident hip and major osteoporotic fractures in older US women with normal or low bone mass.
Copyright © 2011 American Society for Bone and Mineral Research.
Conflict of interest statement
Figures
References
-
- Cummings SR, Nevitt MC, Browner WS, Stone K, Fox KM, Ensrud KE, Cauley J, Black D, Vogt TM. Risk factors for hip fracture in white women. Study of Osteoporotic Fractures Research Group. N Engl J Med. 1995;332:767–773. - PubMed
-
- Hillier TA, Stone KL, Bauer DC, Rizzo JH, Pedula KL, Cauley JA, Ensrud KE, Hochberg MC, Cummings SR. Evaluating the value of repeat bone mineral density measurement and prediction of fractures in older women: The study of osteoporotic fractures. Arch Intern Med. 2007;167:155–160. - PubMed
-
- Siris ES, Chen YT, Abbott TA, Barrett-Connor E, Miller PD, Wehren LE, Berger ML. Bone mineral density thresholds for pharmacological intervention to prevent fractures. Arch Intern Med. 2004;164:1108–1112. - PubMed
-
- Kanis JA, Oden A, Johnell O, Johansson H, De Laet C, Brown J, Burckhardt P, Cooper C, Christiansen C, Cummings S, Eisman JA, Fujiwara S, Gluer C, Goltzman D, Hans D, Krieg MA, La CA, McCloskey E, Mellstrom D, Melton LJ, III, Pols H, Reeve J, Sanders K, Schott AM, Silman A, Torgerson D, van ST, Watts NB, Yoshimura N. The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. Osteoporos Int. 2007;18:1033–1046. - PubMed
-
- Kanis JA, McCloskey EV, Johansson H, Strom O, Borgstrom F, Oden A. Case finding for the management of osteoporosis with FRAX--assessment and intervention thresholds for the UK. Osteoporos Int. 2008;19:1395–1408. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 AR035583/AR/NIAMS NIH HHS/United States
- AR35582/AR/NIAMS NIH HHS/United States
- R01 AR035584/AR/NIAMS NIH HHS/United States
- AG05394/AG/NIA NIH HHS/United States
- R01 AG027576/AG/NIA NIH HHS/United States
- 2 R01 AG027574-22A1/AG/NIA NIH HHS/United States
- R01 AG005407/AG/NIA NIH HHS/United States
- R01 AR035582/AR/NIAMS NIH HHS/United States
- R01 AG005394/AG/NIA NIH HHS/United States
- AR35584/AR/NIAMS NIH HHS/United States
- R01 AG027574/AG/NIA NIH HHS/United States
- 2 R01 AG005394-22A1/AG/NIA NIH HHS/United States
- AG05407/AG/NIA NIH HHS/United States
- R01 AG027576-22/AG/NIA NIH HHS/United States
- AR35583/AR/NIAMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
