

Perianal Crohn's disease findings other than fistulas in a population-based cohort
- PMID: 21351216
- PMCID: PMC3352677
- DOI: 10.1002/ibd.21674
Perianal Crohn's disease findings other than fistulas in a population-based cohort
Abstract
Background: The cumulative incidence of and risk factors for perianal Crohn's disease (CD) for findings other than fistulas are unknown.
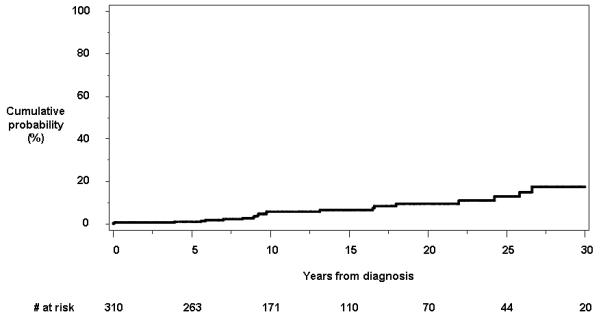
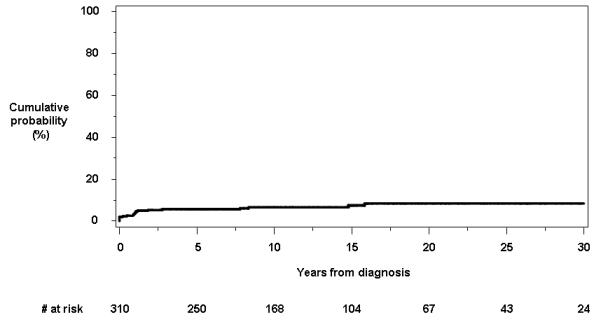
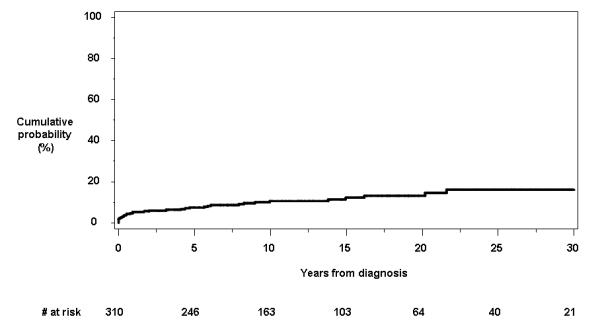
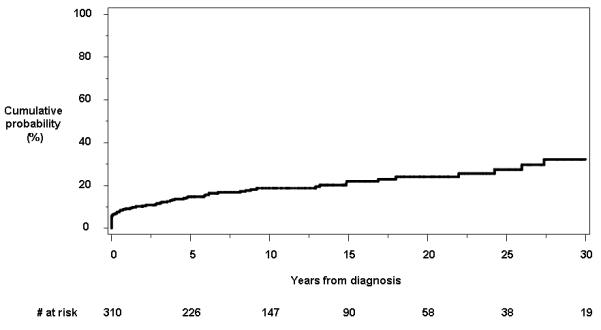
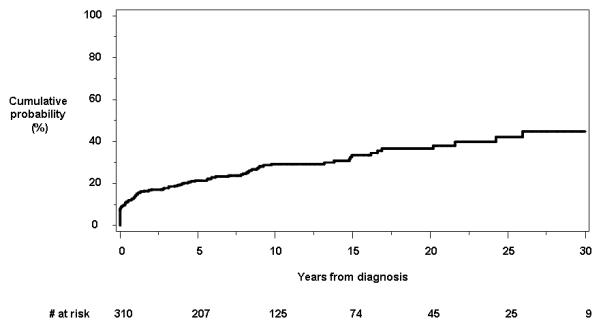
Methods: The medical records of 310 incident cases of CD from Olmsted County, Minnesota, diagnosed between 1970 and 2004, were reviewed for evidence of perianal disease findings other than fistulas. Cumulative incidence was estimated using the Kaplan-Meier method, and associations between baseline factors and time to first event were assessed using proportional hazards regression. Four types of lesions were studied: anorectal strictures, deep anal canal ulcers, anal fissures, and perianal skin tags.
Results: The 10-year cumulative probability from time of diagnosis was 5.8% (95% confidence interval [CI], 2.6%-8.8%) for anorectal strictures, 6.6% (3.6%-9.6%) for deep anal canal ulcers, 10.5% (6.8%-14.1%) for anal fissures, and 18.7% (13.9%-23.3%) for perianal skin tags. The cumulative probability for any perianal lesion other than fistulas was 21.3% (16.5%-25.8%) at 5 years and 29.2% (23.5%-34.5%) at 10 years. Baseline factors associated with time to first perianal lesion other than fistulas were age (hazard ratio [HR] per 10 years, 0.9; 95% CI, 0.8-0.98; P = 0.026), female gender (HR, 1.7; 95% CI, 1.1-2.7; P = 0.013), and presence of extraintestinal manifestations (HR, 1.7; 95% CI, 1.03-2.8; P = 0.038).
Conclusions: Perianal lesions other than fistulas occurred frequently during the clinical course of CD. Female gender and extraintestinal manifestations were associated with increased risks for perianal lesions other than fistulas, while older age at diagnosis was associated with a slightly decreased risk.
Copyright © 2011 Crohn's & Colitis Foundation of America, Inc.
Figures
References
-
- Ingle SB, Loftus EV., Jr The natural history of perianal Crohn’s disease. Dig Liver Dis. 2007;39:963–9. - PubMed
-
- Bouguen G, Siproudhis L, Bretagne JF, Bigard MA, Peyrin-Biroulet L. Nonfistulizing perianal Crohn’s disease: Clinical features, epidemiology, and treatment. Inflamm Bowel Dis. 2010;16:1431–42. - PubMed
-
- Keighley MR, Allan RN. Current status and influence of operation on perianal Crohn’s disease. Int J Colorectal Dis. 1986;1:104–7. - PubMed
-
- Wolff BG, Culp CE, Beart RW, Jr., Ilstrup DM, Ready RL. Anorectal Crohn’s disease. A long-term perspective. Dis Colon Rectum. 1985;28:709–11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical