

Impulse oscillometry in the evaluation of diseases of the airways in children
- PMID: 21354020
- PMCID: PMC3401927
- DOI: 10.1016/j.anai.2010.11.011
Impulse oscillometry in the evaluation of diseases of the airways in children
Abstract
Objective: To provide an overview of impulse oscillometry and its application to the evaluation of children with diseases of the airways.
Data sources: Medline and PubMed search, limited to English language and human disease, with keywords forced oscillation, impulse oscillometry, and asthma.
Study selections: The opinions of the authors were used to select studies for inclusion in this review.
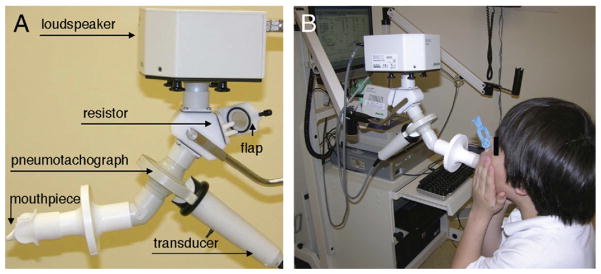
Results: Impulse oscillometry is a noninvasive and rapid technique requiring only passive cooperation by the patient. Pressure oscillations are applied at the mouth to measure pulmonary resistance and reactance. It is employed by health care professionals to help diagnose pediatric pulmonary diseases such asthma and cystic fibrosis; assess therapeutic responses; and measure airway resistance during provocation testing.
Conclusions: Impulse oscillometry provides a rapid, noninvasive measure of airway impedance. It may be easily employed in the diagnosis and management of diseases of the airways in children.
Copyright © 2011 American College of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Impulse oscillometry: pulmonary function assessment in preschool children.Expert Rev Respir Med. 2020 Dec;14(12):1261-1266. doi: 10.1080/17476348.2020.1813573. Epub 2020 Sep 20. Expert Rev Respir Med. 2020. PMID: 32852224
-
Impulse oscillometry in the assessment of children's lung function.Allergol Immunopathol (Madr). 2019 May-Jun;47(3):295-302. doi: 10.1016/j.aller.2018.03.003. Epub 2018 Jul 5. Allergol Immunopathol (Madr). 2019. PMID: 29983239 Review.
-
The case for impulse oscillometry in the management of asthma in children and adults.Ann Allergy Asthma Immunol. 2017 Jun;118(6):664-671. doi: 10.1016/j.anai.2017.04.009. Ann Allergy Asthma Immunol. 2017. PMID: 28583260 Free PMC article. Review.
-
[Standard technical specifications for methacholine chloride (Methacholine) bronchial challenge test (2023)].Zhonghua Jie He He Hu Xi Za Zhi. 2024 Feb 12;47(2):101-119. doi: 10.3760/cma.j.cn112147-20231019-00247. Zhonghua Jie He He Hu Xi Za Zhi. 2024. PMID: 38309959 Chinese.
-
Impulse oscillometry.Adv Respir Med. 2019;87(4):235-238. doi: 10.5603/ARM.a2019.0039. Adv Respir Med. 2019. PMID: 31476011
Cited by
-
Small airway dysfunction and poor asthma control: a dangerous liaison.Clin Mol Allergy. 2021 May 29;19(1):7. doi: 10.1186/s12948-021-00147-8. Clin Mol Allergy. 2021. PMID: 34051816 Free PMC article. Review.
-
A Longitudinal Study of Respiratory Mechanics in Pregnant Women with Obesity and Overweight.Lung. 2023 Aug;201(4):371-379. doi: 10.1007/s00408-023-00633-7. Epub 2023 Jul 8. Lung. 2023. PMID: 37421433
-
Application of Impulse Oscillometry in Adult Asthmatic Patients With Preserved Lung Function.Allergy Asthma Immunol Res. 2020 Sep;12(5):832-843. doi: 10.4168/aair.2020.12.5.832. Allergy Asthma Immunol Res. 2020. PMID: 32638563 Free PMC article.
-
Impulse oscillometry reference values and bronchodilator response in three- to five-year old children living at high altitude.J Asthma Allergy. 2019 Sep 19;12:263-271. doi: 10.2147/JAA.S214297. eCollection 2019. J Asthma Allergy. 2019. PMID: 31571933 Free PMC article.
-
Lung Function Tests in Infants and Children.Indian J Pediatr. 2023 Aug;90(8):790-797. doi: 10.1007/s12098-023-04588-8. Epub 2023 Jun 1. Indian J Pediatr. 2023. PMID: 37261706 Free PMC article. Review.
References
-
- Foliaki S, Annesi-Maesano I, Daniel R, et al. Prevalence of symptoms of childhood asthma, allergic rhinoconjunctivitis and eczema in the Pacific: the International Study of Asthma and Allergies in Childhood (ISAAC) Allergy. 2007;62:259–264. - PubMed
-
- Gerald LB, Sockrider MM, Grad R, et al. An official ATS workshop report: issues in screening for asthma in children. Proc Am Thorac Soc. 2007;4:133–141. - PubMed
-
- Marotta A, Klinnert MD, Price MR, Larsen GL, Liu AH. Impulse oscillometry provides an effective measure of lung dysfunction in 4-year-old children at risk for persistent asthma. J Allergy Clin Immunol. 2003;112:317–322. - PubMed
-
- Neve V, Edme JL, Devos P, et al. Spirometry in 3–5-year-old children with asthma. Pediatr Pulmonol. 2006;41:735–743. - PubMed
-
- Dubois AB, Brody AW, Lewis DH, Burgess BF., Jr Oscillation mechanics of lungs and chest in man. J Appl Physiol. 1956;8:587–594. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
