

Proteomic changes in the heart of diet-induced pre-diabetic mice
- PMID: 21354350
- PMCID: PMC3081671
- DOI: 10.1016/j.jprot.2011.02.018
Proteomic changes in the heart of diet-induced pre-diabetic mice
Abstract
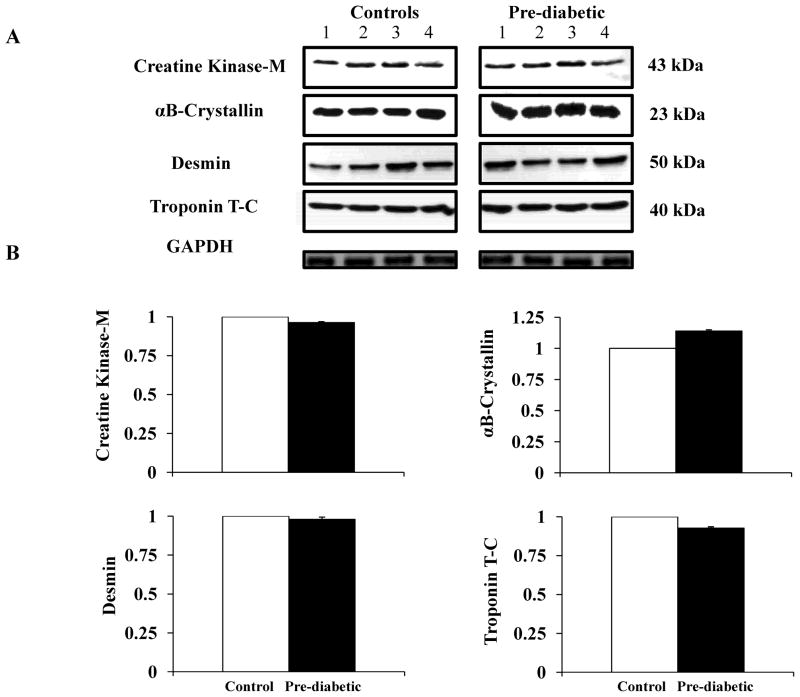
The development of type 2 diabetes (T2D) is strongly associated with obesity. In humans, T2D increases the risk for end organ complications. Among these, heart disease has been ranked as the leading cause of death. We used a proteomic methodology to test the hypothesis that a pre-diabetic state generated by high-fat diet leads to changes in proteins related to heart function and structure. Over 300 protein spots were resolved by two-dimensional gel electrophoresis (2-DE). Fifteen protein spots were found to be altered (7 decreased and 8 increased) in pre-diabetic hearts. The protein spots were then identified by mass spectrometry and immunoblots. Among the decreased proteins, 3 are involved in heart structure (one isoform of desmin, troponin T2 and α-cardiac actin), 3 are involved in energy metabolism (mitochondrial ATP synthase β subunit, adenylate kinase and creatine kinase) and one is a component of the citric acid cycle (isocitrate dehydrogenase 3). In contrast, proteins involved in fatty acid oxidation (two isoforms of peroxisomal enoyl-CoA hydratase) and the citric acid cycle (three isoforms of malate dehydrogenase) were increased in pre-diabetic hearts. The results suggest that changes in the levels of several heart proteins may have implications in the development of the cardiac phenotype associated to T2D.
Copyright © 2011 Elsevier B.V. All rights reserved.
Figures



References
-
- Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States, 2000. Jama. 2004;291:1238–45. - PubMed
-
- Engelgau MM, Geiss LS, Saaddine JB, Boyle JP, Benjamin SM, Gregg EW, et al. The evolving diabetes burden in the United States. Ann Intern Med. 2004;140:945–50. - PubMed
-
- Cowie CC, Rust KF, Byrd-Holt DD, Eberhardt MS, Flegal KM, Engelgau MM, et al. Prevalence of diabetes and impaired fasting glucose in adults in the U.S. population: National Health And Nutrition Examination Survey 1999-2002. Diabetes Care. 2006;29:1263–8. - PubMed
-
- Resnick HE, Harris MI, Brock DB, Harris TB. American Diabetes Association diabetes diagnostic criteria, advancing age, and cardiovascular disease risk profiles: results from the Third National Health and Nutrition Examination Survey. Diabetes Care. 2000;23:176–80. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
