

Clinical utility of real-time fusion guidance for biopsy and ablation
- PMID: 21354816
- PMCID: PMC3071444
- DOI: 10.1016/j.jvir.2010.10.033
Clinical utility of real-time fusion guidance for biopsy and ablation
Abstract
Purpose: To show utility, accuracy, and clinical outcomes of electromagnetic tracking and multimodality image fusion for guidance of biopsy and radiofrequency (RF) ablation procedures.
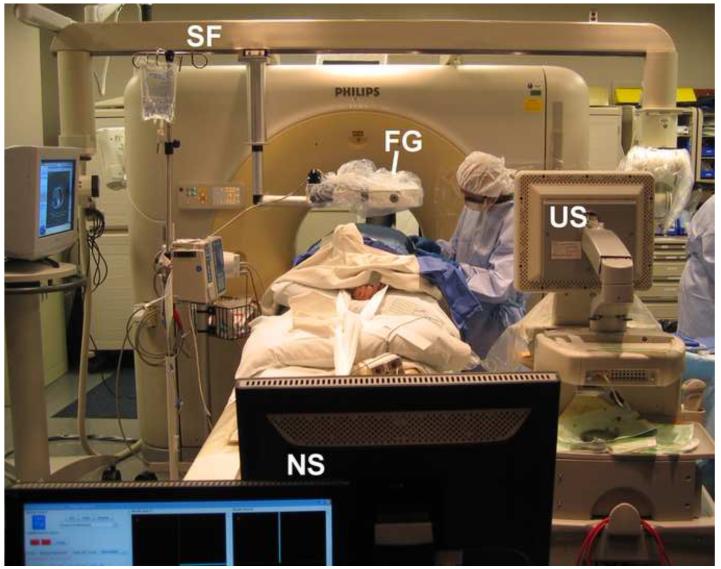
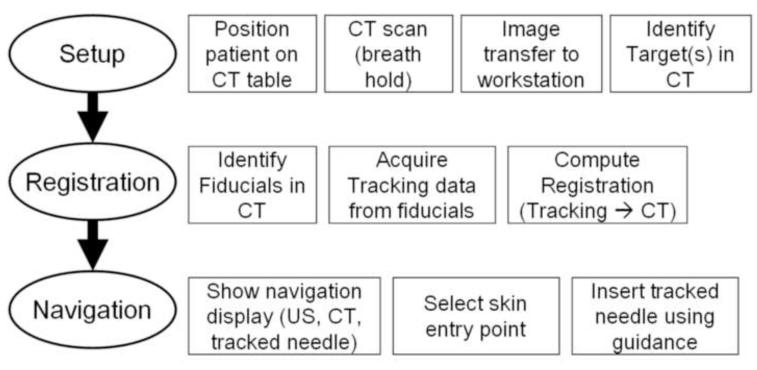
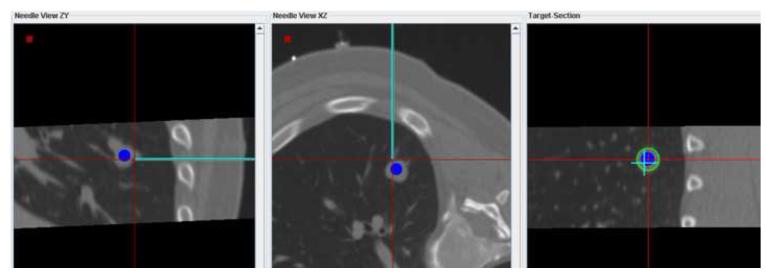
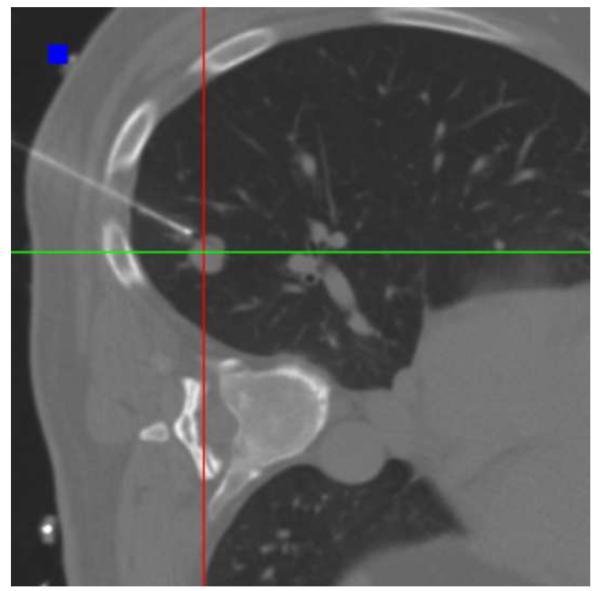
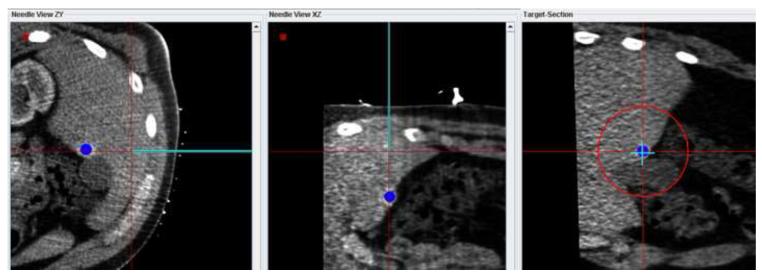
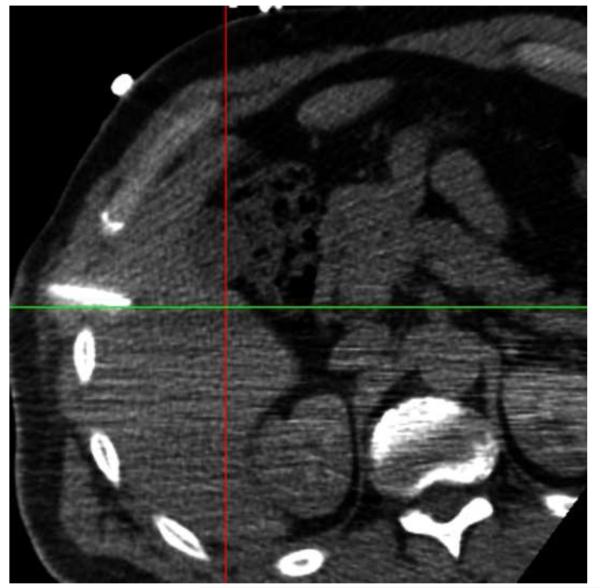
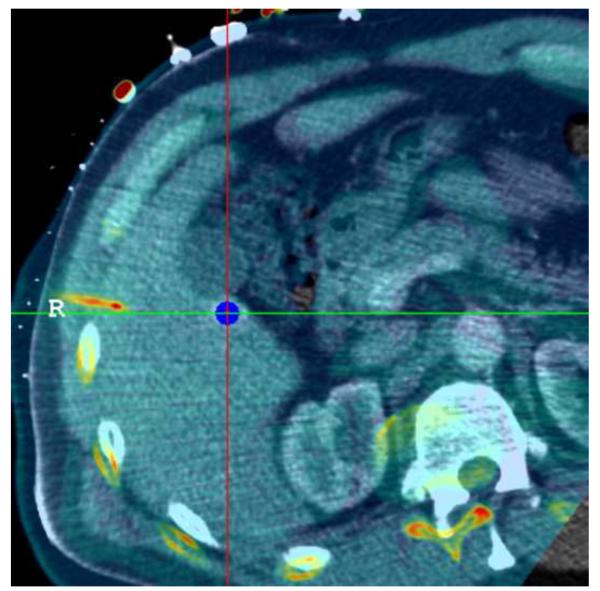
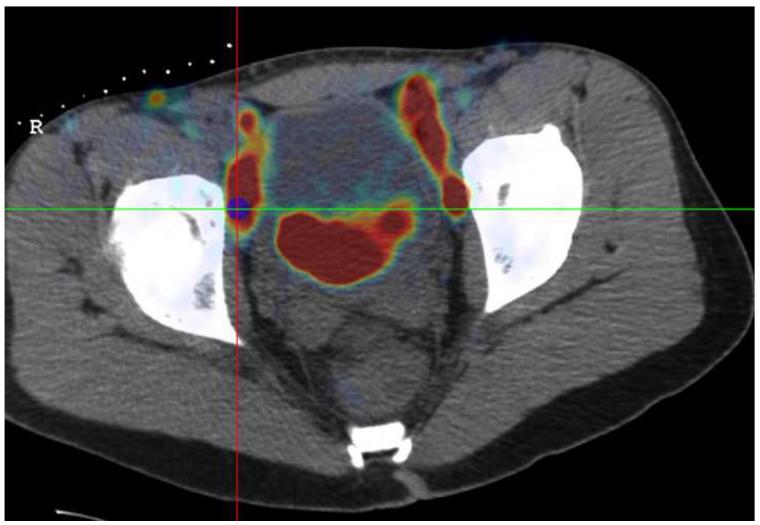
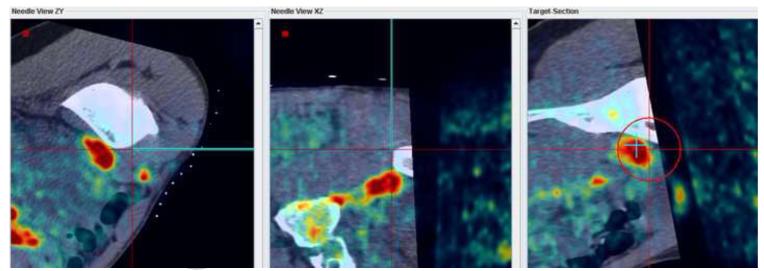
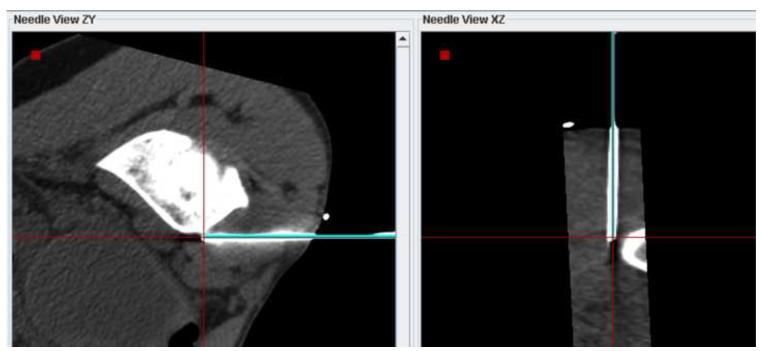
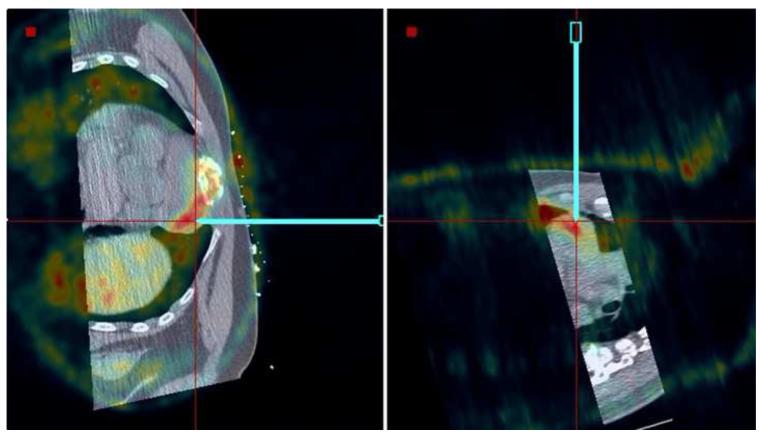
Materials and methods: A combination of conventional image guidance (ultrasound[US]/computed tomography [CT]) and a research navigation system was used in 40 patients undergoing biopsy or RF ablation to assist in target localization and needle and electrode placement. The navigation system displays electromagnetically tracked needles and US images relative to a preprocedural CT scan. Additional images (prior positron emission tomography [PET] or magnetic resonance [MR] imaging) can be fused with CT as needed. Needle aiming with and without tracking were compared, the utility of navigation for each procedure was assessed, the system's off-target tracking error for two different registration methods was evaluated, and setup time was recorded.
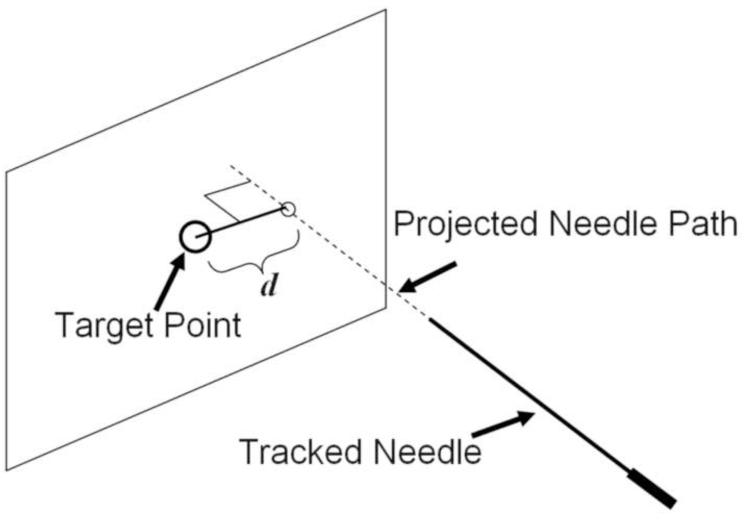
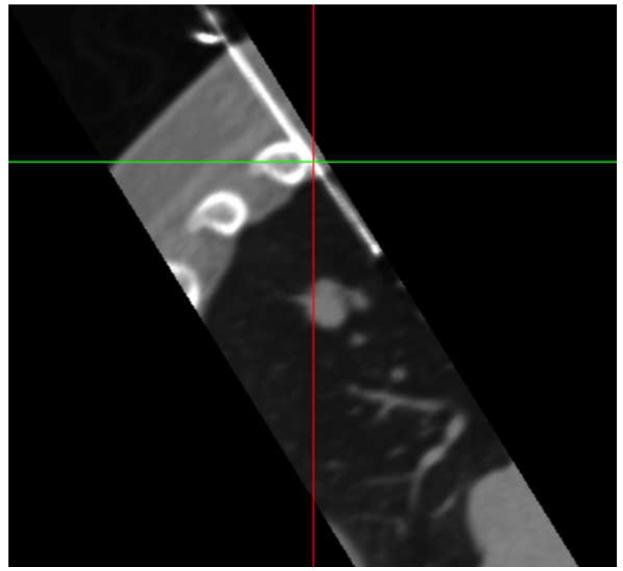
Results: The tracking error could be evaluated in 35 of 40 patients. A basic tracking error of 3.8 mm ± 2.3 was shown using skin fiducial markers for registration. The error improved to 2.7 mm ± 1.6 when using prior internal needle positions as additional fiducial markers. Real-time fusion of US with CT and registration with prior PET and MR imaging were successful and provided clinically relevant guidance information, enabling 19 of the 40 procedures.
Conclusions: The spatial accuracy of the navigation system is sufficient to display clinically relevant image guidance information during biopsy and RF ablation. Breath holding and respiratory gating are effective in minimizing the error associated with tissue motion. In 48% of cases, the navigation system provided information crucial for successful execution of the procedure. Fusion of real-time US with CT or prior diagnostic images may enable procedures that are not feasible with standard, single-modality image guidance.
Trial registration: ClinicalTrials.gov NCT00102544.
Copyright © 2011 SIR. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Goldberg SN, Dupuy DE. Image-guided radiofrequency tumor ablation: challenges and opportunities--part I. J Vasc Interv Radiol. 2001;12:1021–1032. - PubMed
-
- Goldberg SN. Radiofrequency tumor ablation: principles and techniques. Eur J Ultrasound. 2001;13:129–147. - PubMed
-
- Dupuy DE, Goldberg SN. Image-guided radiofrequency tumor ablation: challenges and opportunities--part II. J Vasc Interv Radiol. 2001;12:1135–1148. - PubMed
-
- Boss A, Clasen S, Kuczyk M, et al. Magnetic resonance-guided percutaneous radiofrequency ablation of renal cell carcinomas: a pilot clinical study. Invest Radiol. 2005;40:583–590. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
