

Dissociations between behavioural and functional magnetic resonance imaging-based evaluations of cognitive function after brain injury
- PMID: 21354974
- PMCID: PMC3044833
- DOI: 10.1093/brain/awr005
Dissociations between behavioural and functional magnetic resonance imaging-based evaluations of cognitive function after brain injury
Abstract
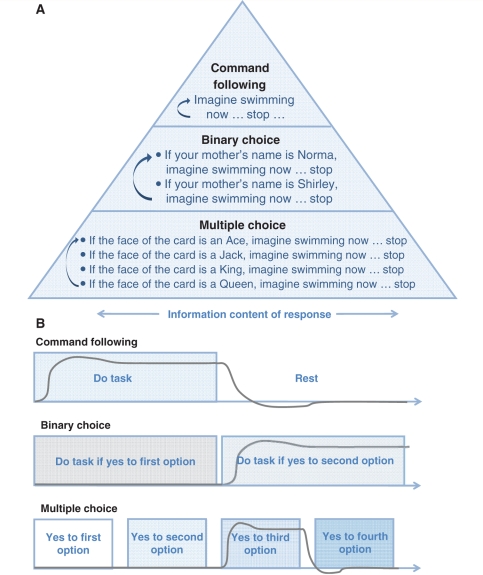
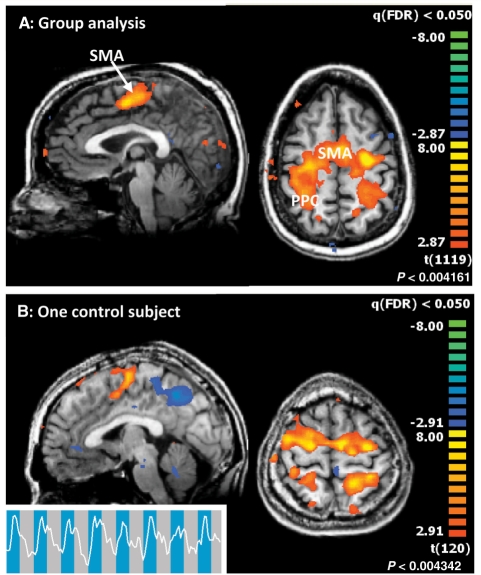
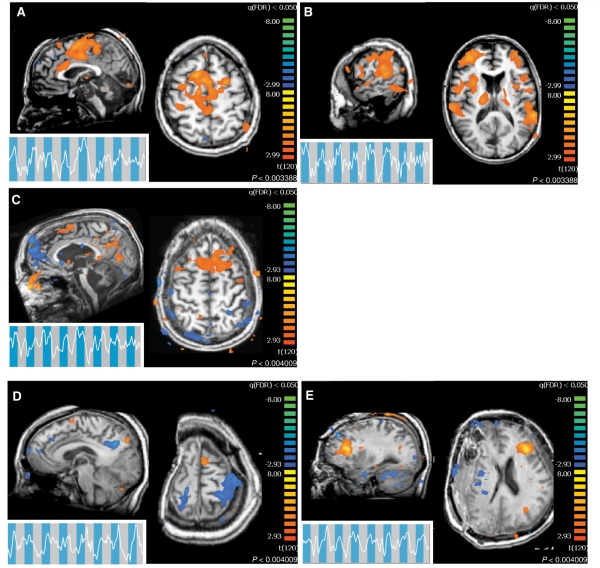
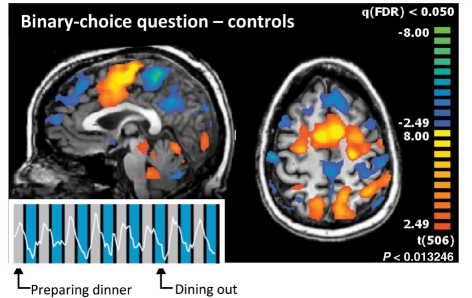
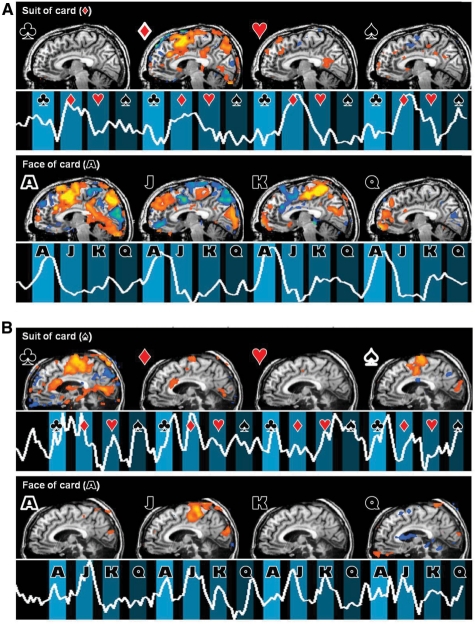
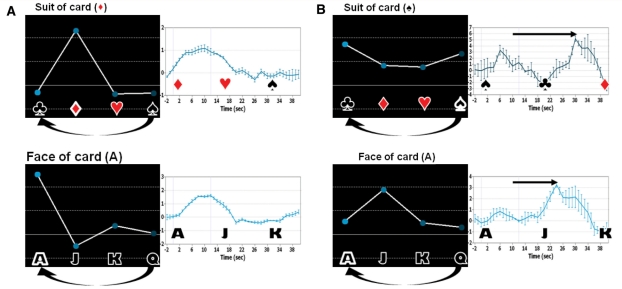
Functional neuroimaging methods hold promise for the identification of cognitive function and communication capacity in some severely brain-injured patients who may not retain sufficient motor function to demonstrate their abilities. We studied seven severely brain-injured patients and a control group of 14 subjects using a novel hierarchical functional magnetic resonance imaging assessment utilizing mental imagery responses. Whereas the control group showed consistent and accurate (for communication) blood-oxygen-level-dependent responses without exception, the brain-injured subjects showed a wide variation in the correlation of blood-oxygen-level-dependent responses and overt behavioural responses. Specifically, the brain-injured subjects dissociated bedside and functional magnetic resonance imaging-based command following and communication capabilities. These observations reveal significant challenges in developing validated functional magnetic resonance imaging-based methods for clinical use and raise interesting questions about underlying brain function assayed using these methods in brain-injured subjects.
Figures
References
-
- Bardin JC, Fins JJ, Hersh J, Heier LA, Schiff ND, Voss HU. Multiple choice fMRI in severely brain injured patients. Neuroscience. 2009 -S-1557-SfN.
-
- Benjamini Y, Hochberg Y. Controlling the false discovery rate––a practical and powerful approach to multiple testing. J R Stat Soc Series B Stat Methodol. 1995;57:289–300.
-
- Boly M, Coleman MR, Davis MH, Hampshire A, Bor D, Moonen G, et al. When thoughts become action: an fMRI paradigm to study volitional brain activity in non-communicative brain injured patients. Neuroimage. 2007;36:979–92. - PubMed
-
- Boly M, Faymonville ME, Peigneux P, Lambermont B, Damas P, Del Fiore G, et al. Auditory processing in severely brain injured patients - differences between the minimally conscious state and the persistent vegetative state. Arch Neurol. 2004;61:233–8. - PubMed
-
- Carrai R, Grippo A, Fossi S, Campolo MC, Lanzo G, Pinto F, et al. Transient post-traumatic locked-in syndrome: A case report and a literature review. Clin Neurophysiol. 2009;39:95–100. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
