

Review
doi: 10.1183/09059180.00011010.
Lymphangioleiomyomatosis: what do we know and what are we looking for?
Affiliations
- PMID: 21357890
- PMCID: PMC3386525
- DOI: 10.1183/09059180.00011010
Item in Clipboard
Review
Lymphangioleiomyomatosis: what do we know and what are we looking for?
Eur Respir Rev.
2011 Mar.
Abstract
Lymphangioleiomyomatosis (LAM) is a rare disease characterised by proliferation of abnormal smooth muscle-like cells (LAM cells) leading to progressive cystic destruction of the lung, lymphatic abnormalities and abdominal tumours. It affects predominantly females and can occur sporadically or in patients with tuberous sclerosis complex. This review describes the recent progress in our understanding of the molecular pathogenesis of the disease and LAM cell biology. It also summarises current therapeutic approaches and the most promising areas of research for future therapeutic strategies.
Conflict of interest statement
None declared.
Figures
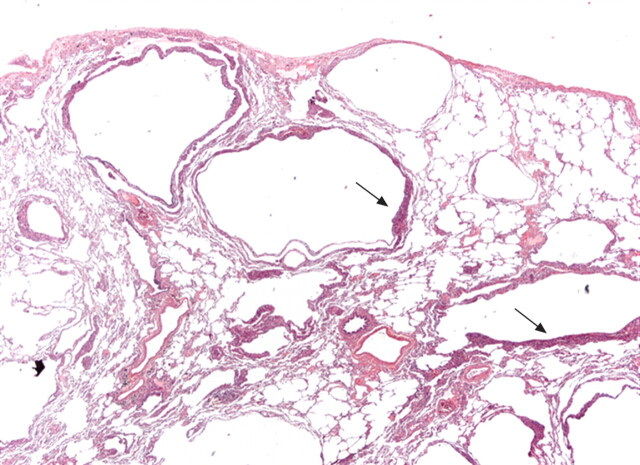
Surgical lung biopsy showing several thin-walled rounded cysts of varying dimensions. The LAM cells form small plaques in the wall of the cysts (arrows) (haematoxylin–eosin, 20×). Figure courtesy of A. Cavazza.
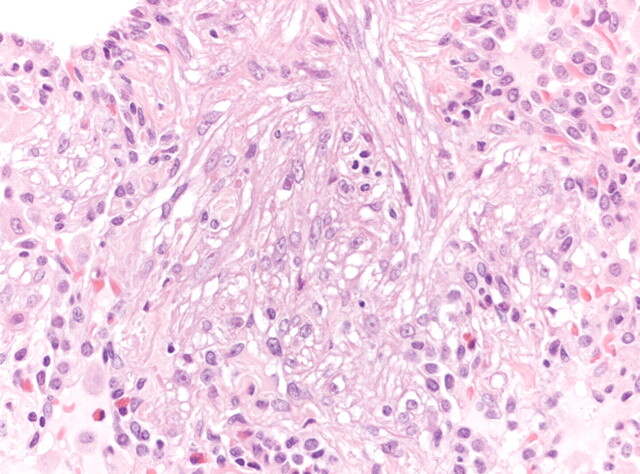
Surgical lung biopsy showing LAM cells. Note the spindle-to-epithelioid morphology, the large amount of eosinophilic cytoplasm and the bland nuclei (haematoxylin–eosin, 200×). Figure courtesy of A. Cavazza.
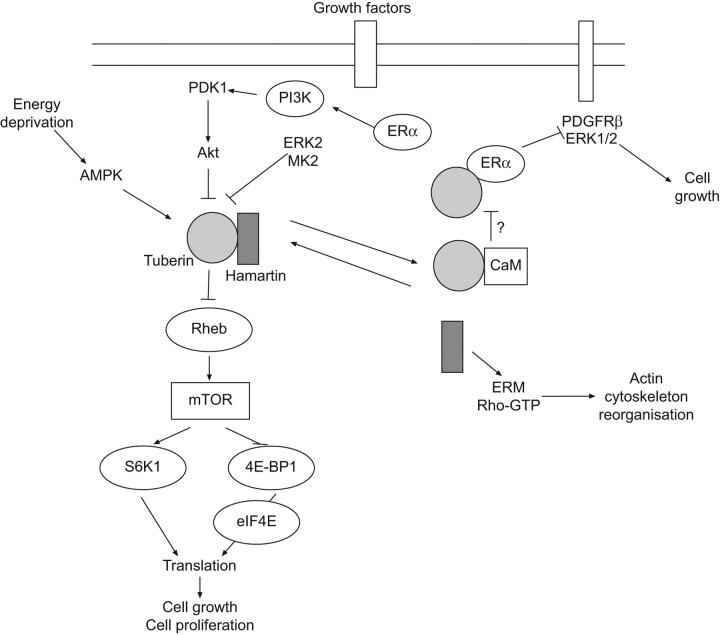
Schematic representation of the signalling transduction pathways involving the tuberous sclerosis proteins, hamartin and tuberin. The main pathway involved in lymphangioleiomyomatosis pathogenesis is mediated by Akt, whose activation inhibits hamartin–tuberin complex, leading to mammalian target of rapamycin (mTOR) activation and thus to cell growth and proliferation. Arrows indicate activating or facilitating influences; flat-headed lines indicate inhibitory influences. ERK2: extracellular signal-regulated kinase 2; MK2: mitogen-activated protein kinase (MAPK)-activated protein kinase 2; Rheb: Ras homologue expressed in brain; ERα: oestrogen receptor α; PDGFRβ: platelet-derived growth factor receptor β; CaM: calmodulin; ERM: ezrin-radixin-moesin.
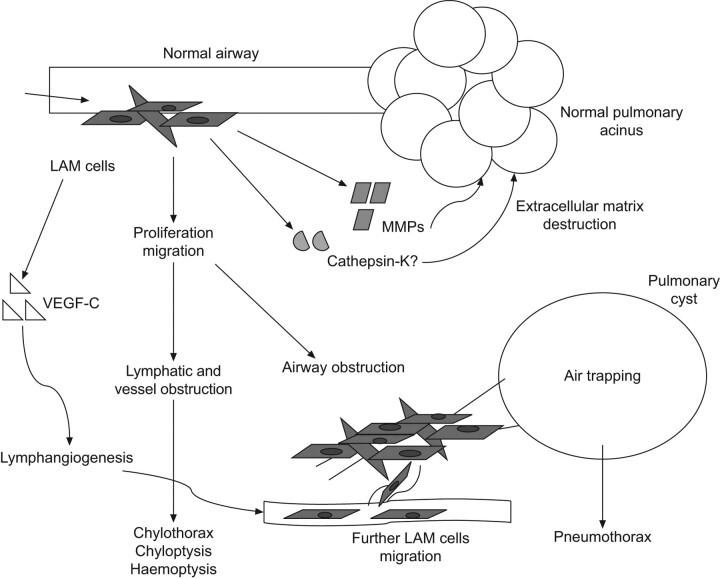
Possible mechanisms of lung cysts formation in lymphangioleiomyomatosis (LAM). VEGF: vascular endothelial growth factor; MMP: matrix metalloproteinase. Adapted from [76] with permission from the publisher.

Chest radiograph in lymphangioleiomyomatosis showing bilateral reticular changes.

Chest radiograph in lymphangioleiomyomatosis showing bilateral pleural effusion and interstitial changes. Thoracentesis confirmed the presence of chylous pleural effusion.
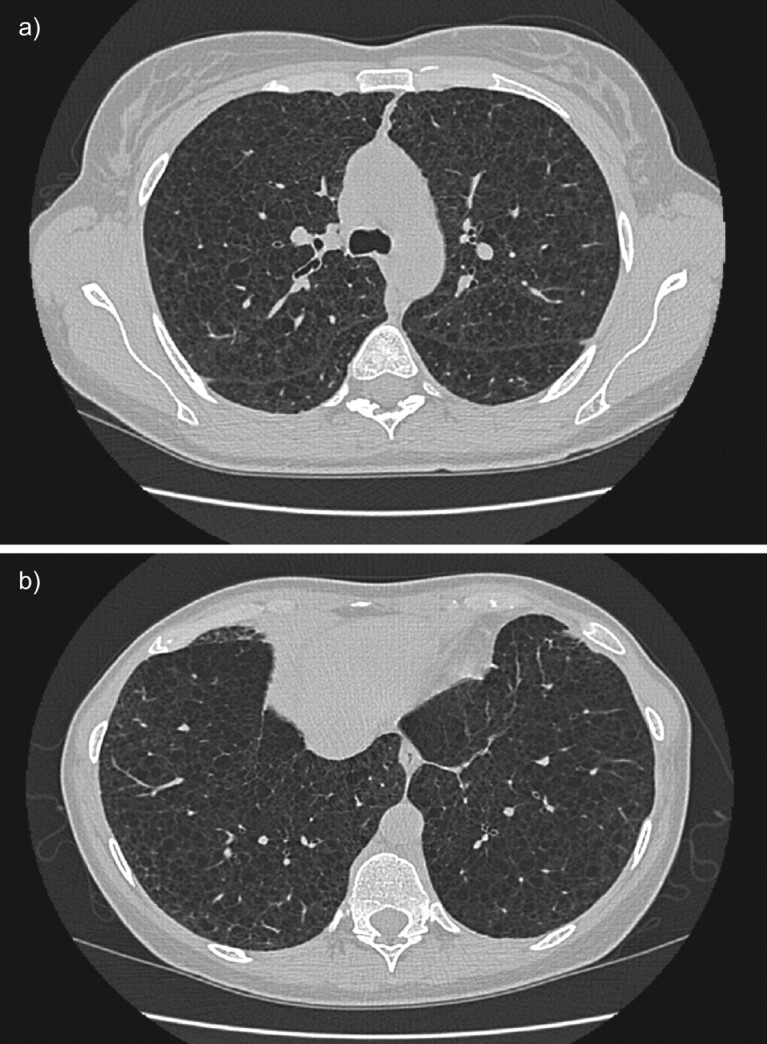
High-resolution computed tomography scans of the chest in a patient with histological diagnosis of lymphangioleiomyomatosis. Round shaped, thin-walled cysts are distributed diffusely throughout the lungs (a) without sparing of lung bases (b).
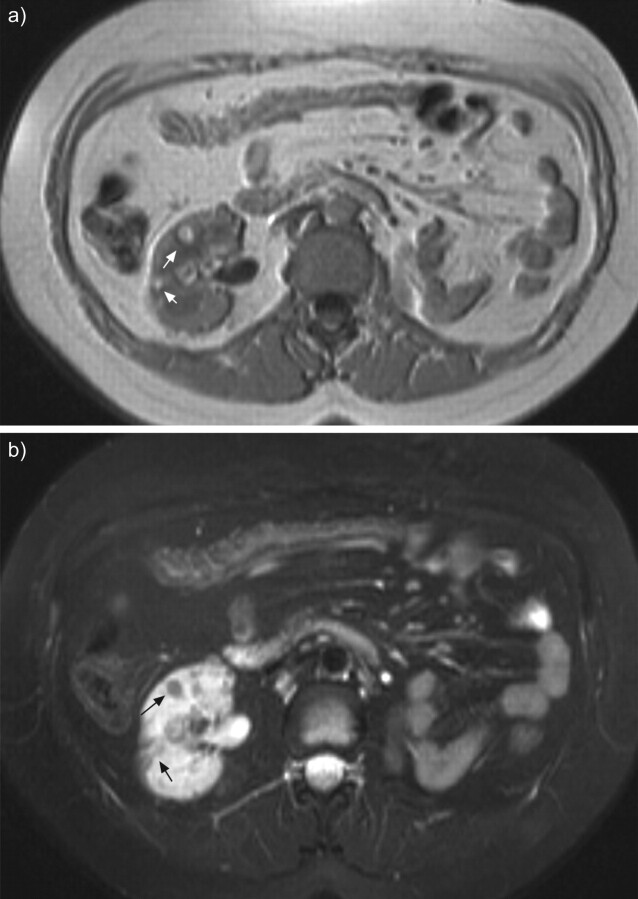
Abdominal magnetic resonance imaging of a patient with tuberous sclerosis complex lymphangioleiomyomatosis and multiple small renal angiomyolipomas (arrows) in T1-weighted images (a) and fat suppression signal sequences (b). Left nephrectomy was performed for a large angiomyolipoma.
Comment in
-
Milestones in lymphangioleiomyomatosis research.Eur Respir Rev. 2011 Mar;20(119):3-6. doi: 10.1183/09059180.00000311. Eur Respir Rev. 2011. PMID: 21357887 Free PMC article. No abstract available.
References
-
- Kitaichi M, Nishimura K, Itoh H, et al. . Pulmonary lymphangiomyomatosis: a report of 46 patients including a clinicopathologic study of prognostic factors. Am J Respir Crit Care Med 1995; 151: 527–533. - PubMed
-
- Urban T, Lazor R, Lacronique J, et al. . Pulmonary lymphangioleiomyomatosis: a study of 69 patients. Groupe d'Etudes et de Recherche sur les Maladies “Orphelines” Pulmonaires (GERM“O”P). Medicine (Baltimore) 1999; 78: 321–337. - PubMed
-
- Chu SC, Horiba K, Usuki J, et al. . Comprehensive evaluation of 35 patients with lymphangioleiomyomatosis. Chest 1999; 115: 1041–1052. - PubMed