

Receiving early mobility during an intensive care unit admission is a predictor of improved outcomes in acute respiratory failure
- PMID: 21358312
- PMCID: PMC3082620
- DOI: 10.1097/MAJ.0b013e31820ab4f6
Receiving early mobility during an intensive care unit admission is a predictor of improved outcomes in acute respiratory failure
Abstract
Introduction: Hospitals are under pressure to provide care that not only shortens hospital length of stay but also reduces subsequent hospital admissions. Hospital readmissions have received increased attention in outcome reporting. The authors identified survivors of acute respiratory failure who then required subsequent hospitalization. A cohort of acute respiratory failure survivors, who participated in an early intensive care unit (ICU) mobility program, was assessed to determine if variables from the index hospitalization predict hospital readmission or death, within 12 months of hospital discharge.
Methods: Hospital database and responses to letters mailed to 280 acute respiratory failure survivors. Univariate predictor variables shown to be associated with hospital readmission or death (P < 0.1) were included in a multiple logistic regression. A stepwise selection procedure was used to identify significant variables (P < 0.05).
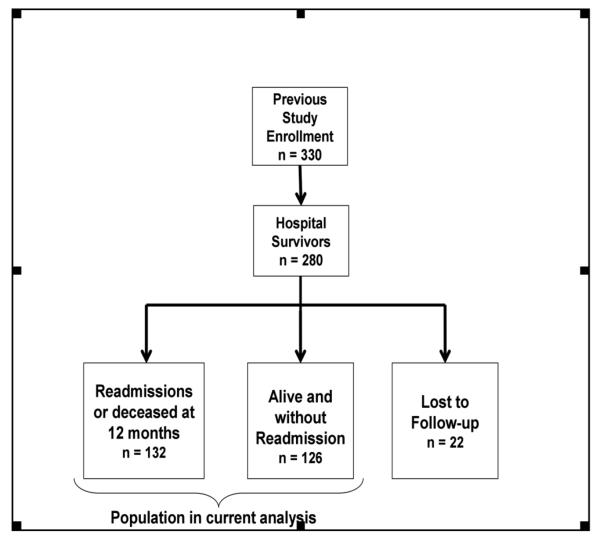
Results: Of the 280 survivors, 132 (47%) had at least 1 readmission or died within the first year, 126 (45%) were not readmitted and 22 (8%) were lost to follow-up. Tracheostomy [odds ratio (OR), 4.02 (95%CI, 1.72-9.40)], female gender [OR, 1.94 (95%CI, 1.13-3.32)], a higher Charlson Comorbidity Index assessed upon index hospitalization discharge [OR, 1.15 (95%CI, 1.01-1.31)] and lack of early ICU mobility therapy [OR, 1.77 (95%CI, 1.04-3.01)] predicted readmission or death in the first year postindex hospitalization.
Conclusions: Tracheostomy, female gender, higher Charlson Comorbidity Index and lack of early ICU mobility were associated with readmissions or death during the first year. Although the mechanisms of increased hospital readmission are unclear, these findings may provide further support for early ICU mobility for patients with acute respiratory failure.
Figures
References
-
- Gonseth J, Guallar-Castillon P, Banegas JR, et al. The effectiveness of disease management programmes in reducing hospital re-admission in older patients with heart failure: a systematic review and meta-analysis of published reports. Eur Heart J. 2004;25(18):1570–1595. - PubMed
-
- Hauptman PJ, Rich MW, Heidenreich PA, et al. The heart failure clinic: a consensus statement of the Heart Failure Society of America. J Card Fail. 2008;14(10):801–815. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418–1428. - PubMed
-
- Hernandez C, Jansa M, Vidal M, et al. The burden of chronic disorders on hospital admissions prompts the need for new modalities of care: A cross-sectional analysis in a tertiary hospital. QJM. 2009;102(3):193–202. - PubMed
-
- Morris PE, Goad A, Thompson C, et al. Early ICU Mobility Therapy in the Treatment of Acute Respiratory Failure. Crit Care Med. 2008;36:2238–2243. - PubMed
