

Autoantibodies against 3-hydroxy-3-methylglutaryl-coenzyme A reductase in patients with statin-associated autoimmune myopathy
- PMID: 21360500
- PMCID: PMC3335400
- DOI: 10.1002/art.30156
Autoantibodies against 3-hydroxy-3-methylglutaryl-coenzyme A reductase in patients with statin-associated autoimmune myopathy
Abstract
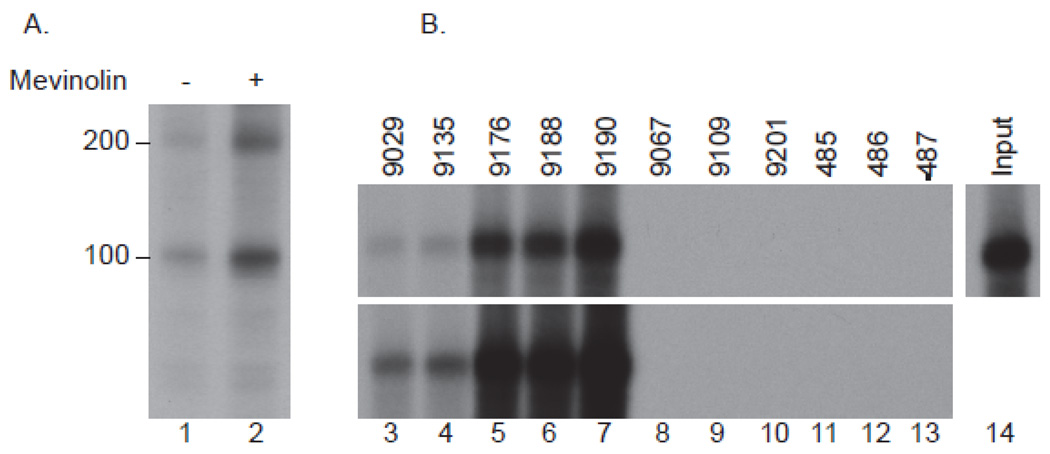
Objective: In addition to inducing a self-limited myopathy, statin use is associated with an immune-mediated necrotizing myopathy (IMNM), with autoantibodies that recognize ∼200-kd and ∼100-kd autoantigens. The purpose of this study was to identify these molecules to help clarify the disease mechanism and facilitate diagnosis.
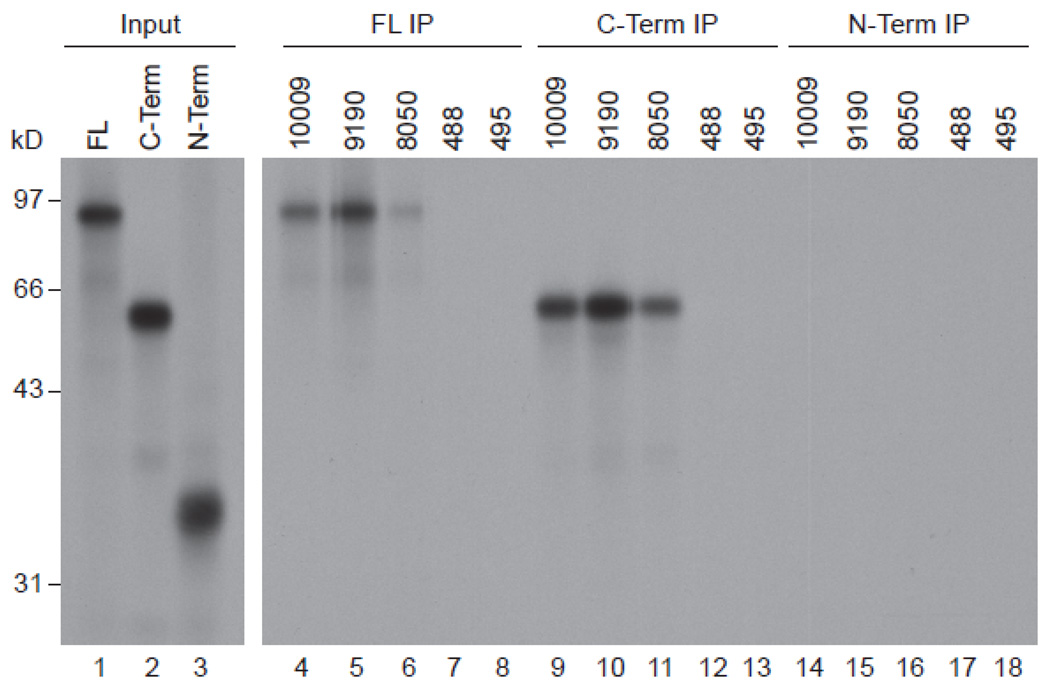
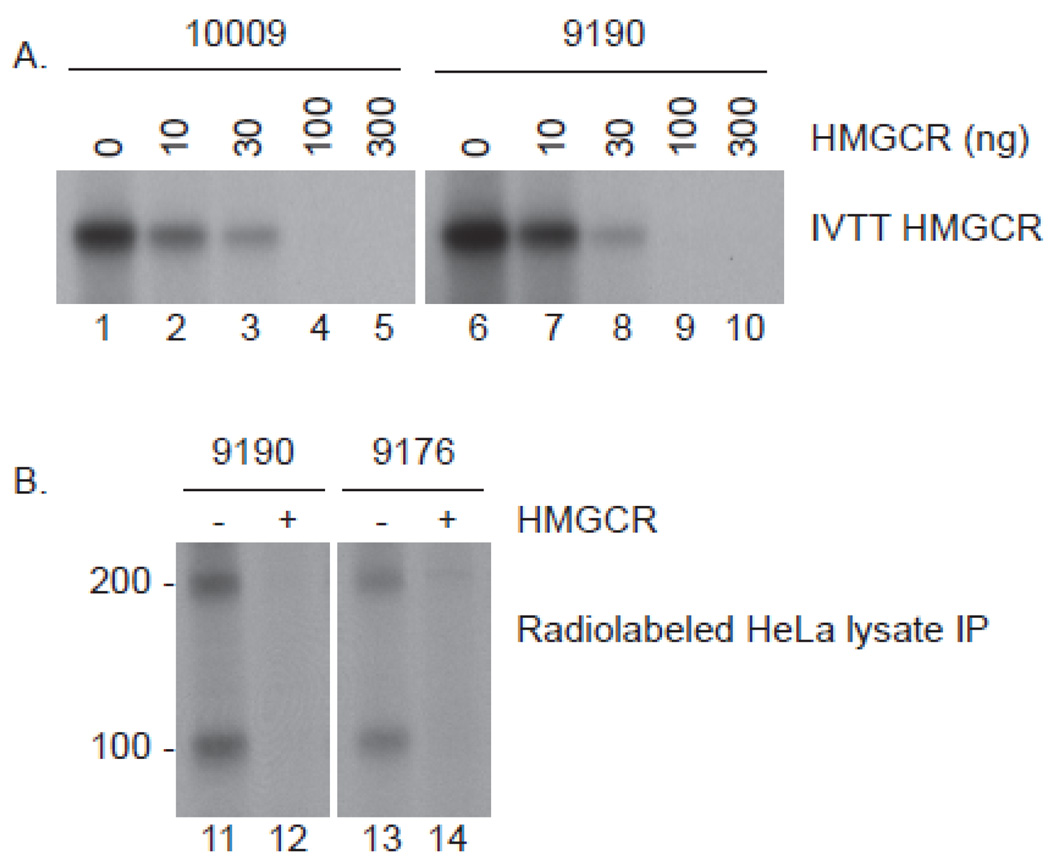
Methods: The effect of statin treatment on autoantigen expression was addressed by immunoprecipitation using sera from patients. The identity of the ∼100-kd autoantigen was confirmed by immunoprecipitation of in vitro-translated 3-hydroxy-3-methylglutaryl-coenzyme A reductase (HMGCR) protein. HMGCR expression in muscle was analyzed by immunofluorescence. A cohort of myopathy patients was screened for anti-HMGCR autoantibodies by enzyme-linked immunosorbent assay and genotyped for the rs4149056 C allele, a predictor of self-limited statin myopathy.
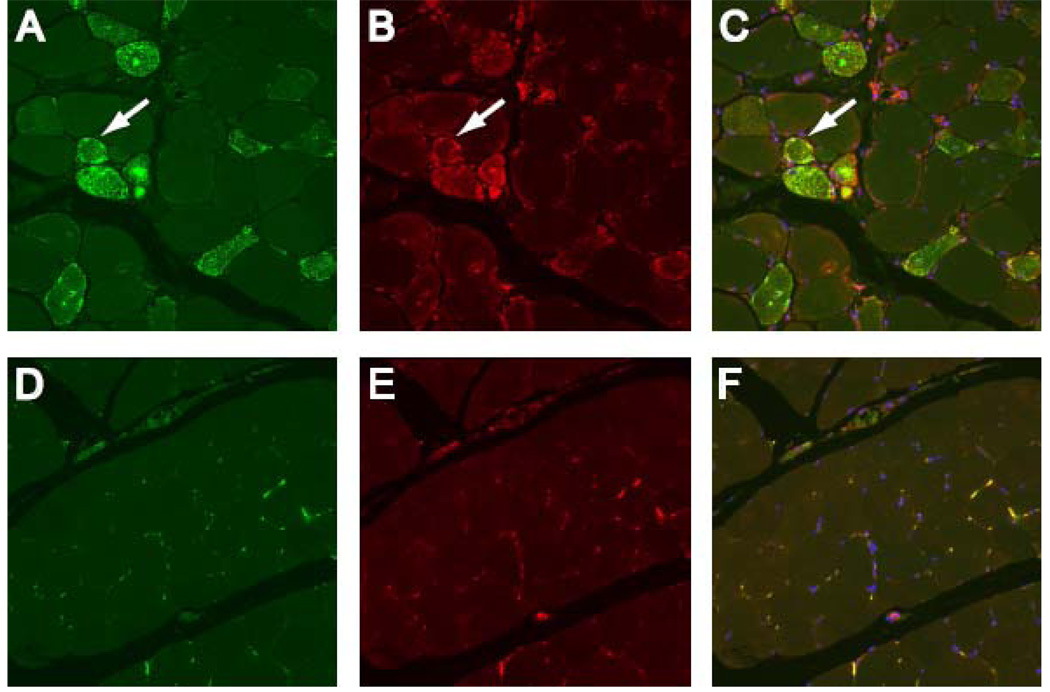
Results: Statin exposure induced expression of the ∼200-kd/∼100-kd autoantigens in cultured cells. HMGCR was identified as the ∼100-kd autoantigen. Competition experiments demonstrated no distinct autoantibodies recognizing the ∼200-kd protein. In muscle biopsy tissues from anti-HMGCR-positive patients, HMGCR expression was up-regulated in cells expressing neural cell adhesion molecule, a marker of muscle regeneration. Anti-HMGCR autoantibodies were found in 45 of 750 patients presenting to the Johns Hopkins Myositis Center (6%). Among patients ages 50 years and older, 92.3% had taken statins. The prevalence of the rs4149056 C allele was not increased in patients with anti-HMGCR.
Conclusion: Statins up-regulate the expression of HMGCR, the major target of autoantibodies in statin-associated IMNM. Regenerating muscle cells express high levels of HMGCR, which may sustain the immune response even after statins are discontinued. These studies demonstrate a mechanistic link between an environmental trigger and the development of sustained autoimmunity. Detection of anti-HMGCR autoantibodies may facilitate diagnosis and direct therapy.
Copyright © 2011 by the American College of Rheumatology.
Figures
References
-
- Statistical brief #205. Trends in statins utilization and expenditures for the U.S. civilian noninstitutionalized population, 2000 and 2005. [July 26, 2010]. Available at: http://www.meps.ahrq.gov/mepsweb/data_files/publications/st205/stat205.pdf.
-
- de Sauvage Nolting PR, Buirma RJ, Hutten BA, Kastelein JJ Dutch ExPRESS Investigator Group. Two-year efficacy and safety of simvastatin 80 mg in familial hypercholesterolemia (the Examination of Probands and Relatives in Statin Studies With Familial Hypercholesterolemia [ExPRESS FH]) Am J Cardiol. 2002 Jul 15;90(2):181–184. - PubMed
-
- Bruckert E, Hayem G, Dejager S, Yau C, Begaud B. Mild to moderate muscular symptoms with high-dosage statin therapy in hyperlipidemic patients--the PRIMO study. Cardiovasc Drugs Ther. 2005 Dec;19(6):403–414. - PubMed
-
- Franc S, Dejager S, Bruckert E, Chauvenet M, Giral P, Turpin G. A comprehensive description of muscle symptoms associated with lipid-lowering drugs. Cardiovasc Drugs Ther. 2003 Sep–Nov;17(5–6):459–465. - PubMed
-
- Graham DJ, Staffa JA, Shatin D, Andrade SE, Schech SD, La Grenade L, et al. Incidence of hospitalized rhabdomyolysis in patients treated with lipid-lowering drugs. JAMA. 2004 Dec 1;292(21):2585–2590. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
