

Augmented therapy improves outcome for pediatric high risk acute lymphocytic leukemia: results of Children's Oncology Group trial P9906
- PMID: 21360654
- PMCID: PMC3136564
- DOI: 10.1002/pbc.22944
Augmented therapy improves outcome for pediatric high risk acute lymphocytic leukemia: results of Children's Oncology Group trial P9906
Abstract
Background: The augmented BFM regimen improves outcome for children with NCI high acute lymphoblastic leukemia (ALL). Patient age, sex, and presenting white blood cell count (WBC) can be used to identify a subset of approximately 12% of children with B-precursor ALL that had a 5-year continuous complete remission (CCR) rate of only about 50% on earlier Pediatric Oncology Group (POG) trials.
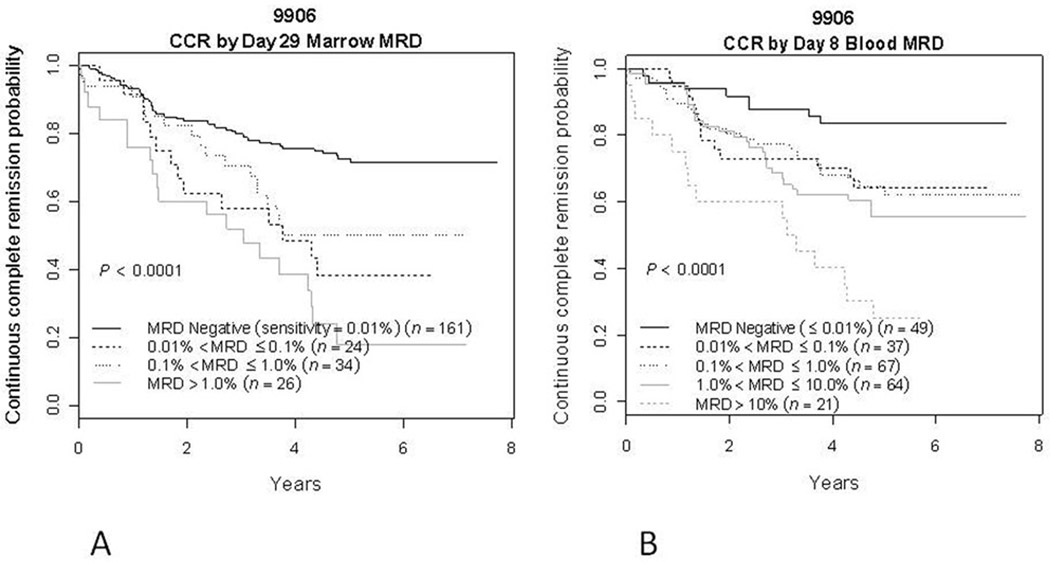
Procedures: Children's Oncology Group trial P9906 evaluated a modified augmented BFM regimen in 267 patients with particularly high risk B-precursor ALL. Minimal residual disease (MRD) was assessed in blood at day 8 and in marrow at day 29 of induction and correlated with outcome.
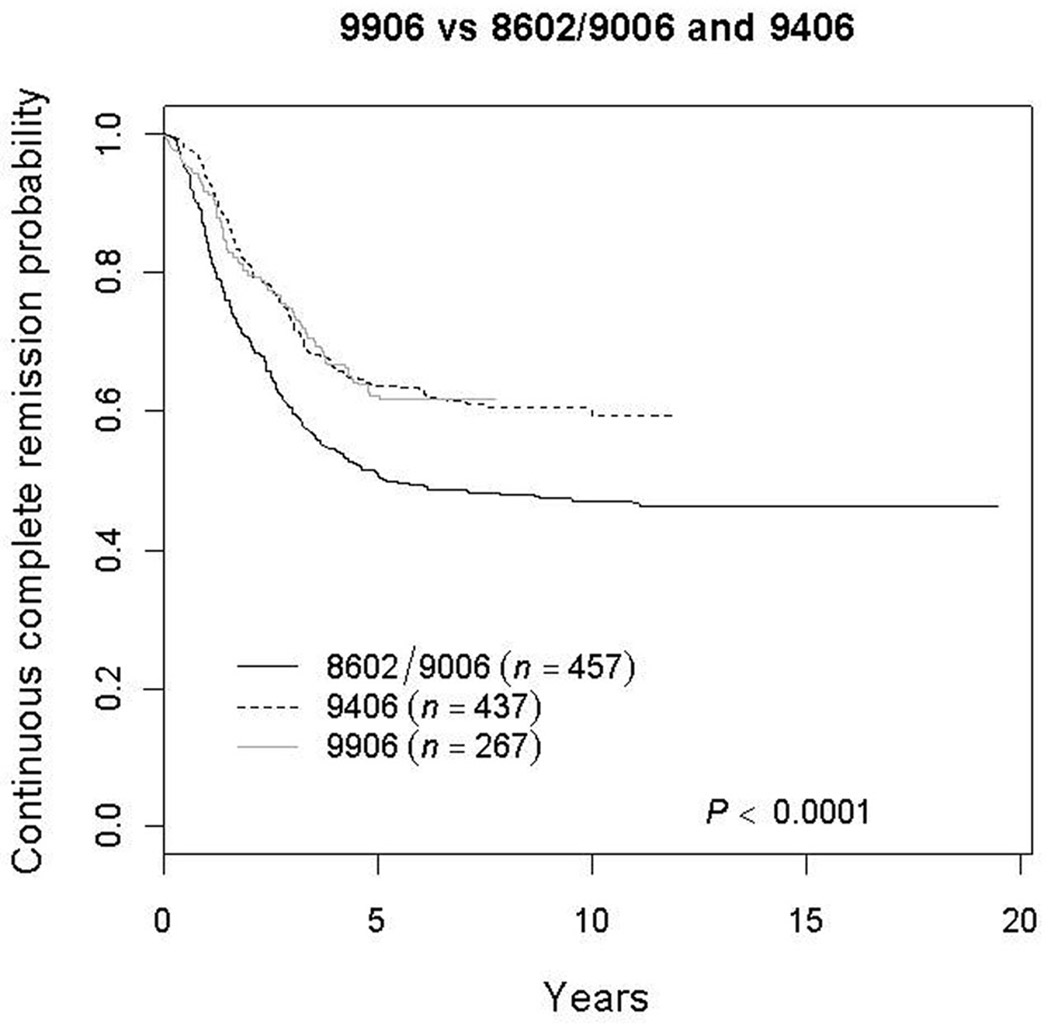
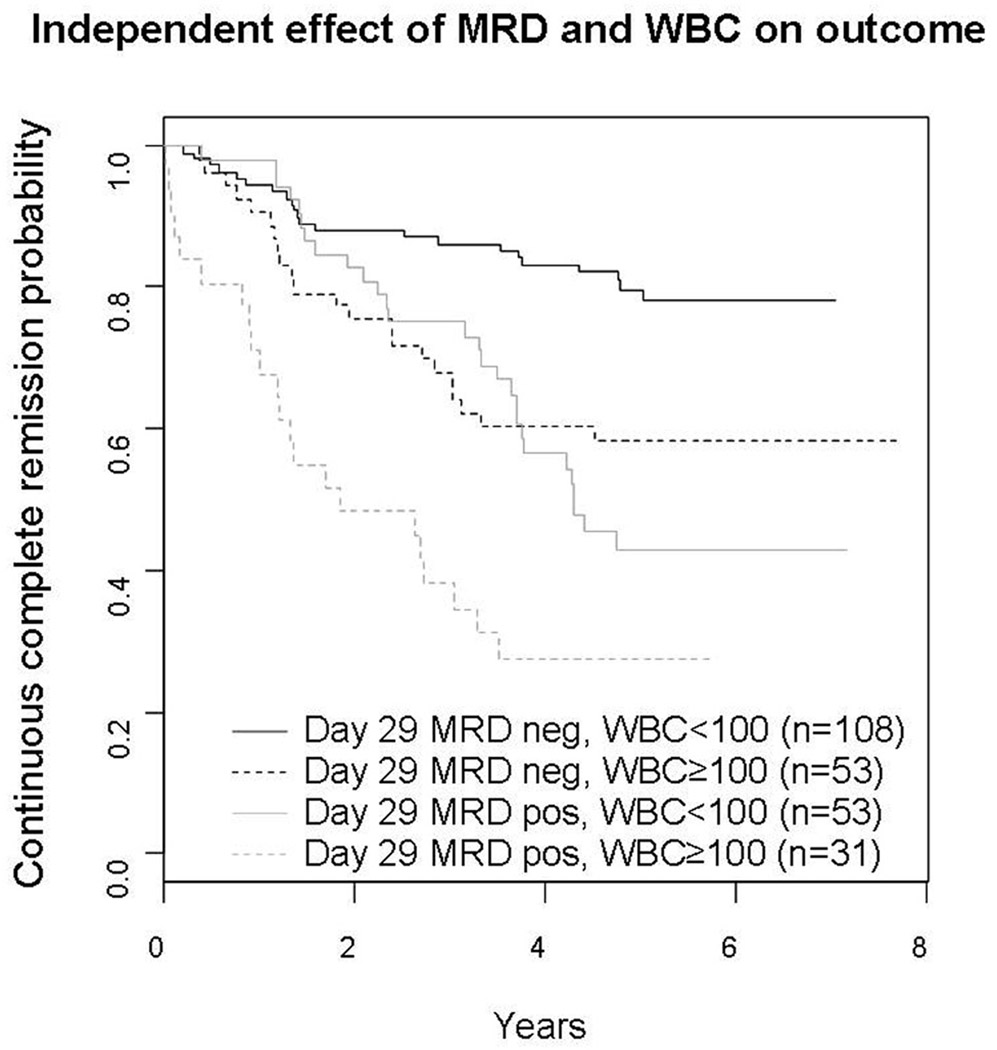
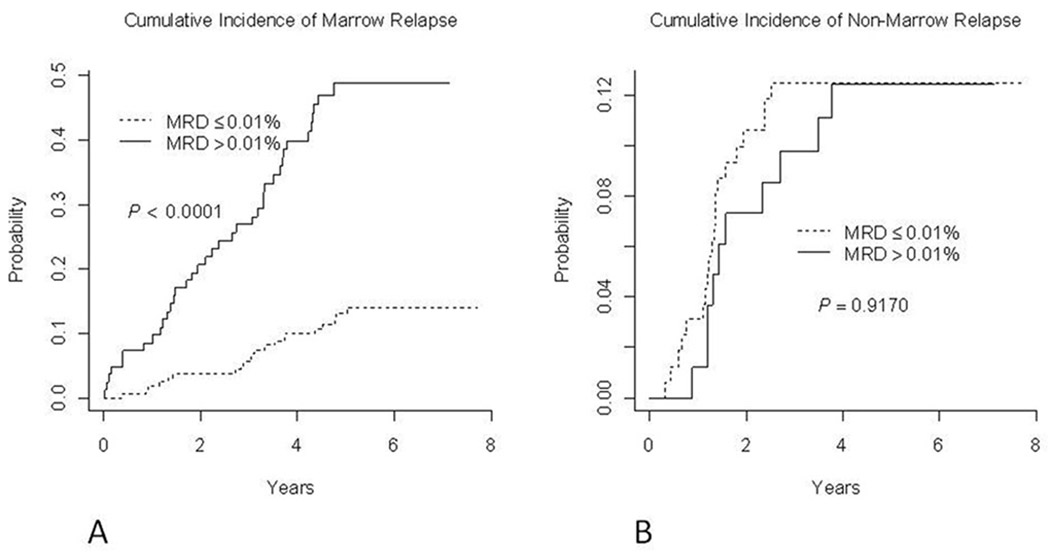
Results: The 5-year CCR probability for patients in P9906 was significantly better than that observed for similar patients on POG trials 8602/9006 (62.2 ± 3.7% vs. 50.6 ± 2.4%; P = 0.0007) but similar to POG 9406 (63.5 ± 2.4%; P = 0.81). Interim analysis showed poor central nervous system (CNS) control, especially in patients with initial WBC ≥ 100,000/microliter. Day 29 marrow MRD positive (≥ 0.01%) vs. negative patients had 5 year CCR rates of 37.1 ± 7.4% vs. 72.6 ± 4.3%; day 8 blood MRD positive vs. negative patients had 5 year CCR rates of 57.1 ± 4.6% vs.83.6 ± 6.3%. End induction marrow MRD predicted marrow but not CNS relapse. In multivariate analysis, day 29 MRD > 0.01%, initial WBC ≥ 100,000/µl, male gender, and day 8 blood MRD > 0.01% were significant prognostic factors.
Conclusions: Augmented BFM therapy improved outcome for children with higher risk ALL. Day 8 blood and day 29 marrow MRD were strong prognostic factors in these patients.
Copyright © 2011 Wiley-Liss, Inc.
Figures
References
-
- Conter V, Arico M, Basso G, et al. Long-term results of the Italian Association of Pediatric Hematology and Oncology (AIEOP) Studies 82, 87, 88, 91 and 95 for childhood acute lymphoblastic leukemia. Leukemia. 2010;24:255–264. - PubMed
-
- Moricke A, Zimmermann M, Reiter A, et al. Long-term results of five consecutive trials in childhood acute lymphoblastic leukemia performed by the ALL-BFM study group from 1981 to 2000. Leukemia. 2010;24:265–284. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
