

Stem and progenitor cell-based therapy in ischaemic heart disease: promise, uncertainties, and challenges
- PMID: 21362705
- PMCID: PMC3094549
- DOI: 10.1093/eurheartj/ehr018
Stem and progenitor cell-based therapy in ischaemic heart disease: promise, uncertainties, and challenges
Abstract
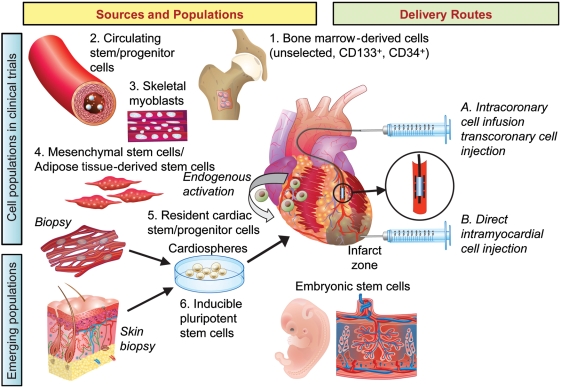
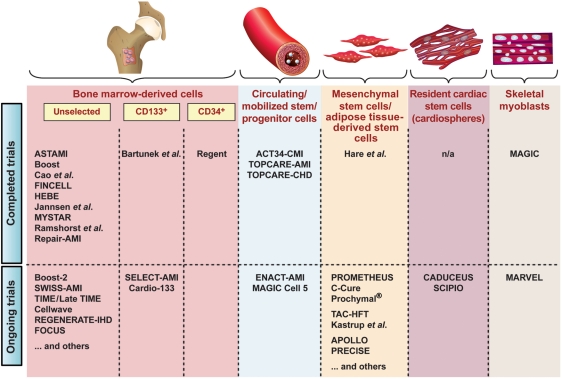
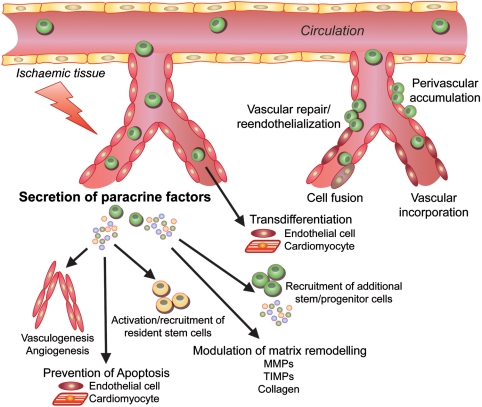
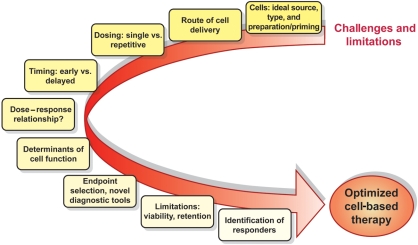
In the absence of effective endogenous repair mechanisms after cardiac injury, cell-based therapies have rapidly emerged as a potential novel therapeutic approach in ischaemic heart disease. After the initial characterization of putative endothelial progenitor cells and their potential to promote cardiac neovascularization and to attenuate ischaemic injury, a decade of intense research has examined several novel approaches to promote cardiac repair in adult life. A variety of adult stem and progenitor cells from different sources have been examined for their potential to promote cardiac repair and regeneration. Although early, small-scale clinical studies underscored the potential effects of cell-based therapy largely by using bone marrow (BM)-derived cells, subsequent randomized-controlled trials have revealed mixed results that might relate, at least in part, to differences in study design and techniques, e.g. differences in patient population, cell sources and preparation, and endpoint selection. Recent meta-analyses have supported the notion that administration of BM-derived cells may improve cardiac function on top of standard therapy. At this stage, further optimization of cell-based therapy is urgently needed, and finally, large-scale clinical trials are required to eventually proof its clinical efficacy with respect to outcomes, i.e. morbidity and mortality. Despite all promises, pending uncertainties and practical limitations attenuate the therapeutic use of stem/progenitor cells for ischaemic heart disease. To advance the field forward, several important aspects need to be addressed in carefully designed studies: comparative studies may allow to discriminate superior cell populations, timing, dosing, priming of cells, and delivery mode for different applications. In order to predict benefit, influencing factors need to be identified with the aim to focus resources and efforts. Local retention and fate of cells in the therapeutic target zone must be improved. Further understanding of regenerative mechanisms will enable optimization at all levels. In this context, cell priming, bionanotechnology, and tissue engineering are emerging tools and may merge into a combined biological approach of ischaemic tissue repair.
Figures
References
-
- Fang J, Mensah GA, Croft JB, Keenan NL. Heart failure-related hospitalization in the U.S., 1979 to 2004. J Am Coll Cardiol. 2008;52:428–434. doi:10.1016/j.jacc.2008.03.061. - DOI - PubMed
-
- Gheorghiade M, Bonow RO. Chronic heart failure in the United States: a manifestation of coronary artery disease. Circulation. 1998;97:282–289. - PubMed
-
- Asahara T, Murohara T, Sullivan A, Silver M, van der Zee R, Li T, Witzenbichler B, Schatteman G, Isner JM. Isolation of putative progenitor endothelial cells for angiogenesis. Science. 1997;275:964–967. doi:10.1126/science.275.5302.964. - DOI - PubMed
-
- Hirschi KK, Ingram DA, Yoder MC. Assessing identity, phenotype, and fate of endothelial progenitor cells. Arterioscler Thromb Vasc Biol. 2008;28:1584–1595. doi:10.1161/ATVBAHA.107.155960. - DOI - PMC - PubMed
-
- Aicher A, Zeiher AM, Dimmeler S. Mobilizing endothelial progenitor cells. Hypertension. 2005;45:321–325. doi:10.1161/01.HYP.0000154789.28695.ea. - DOI - PubMed
